 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 11-16 Selection of Ideal Candidates for Epilepsy Surgery in Developing Countries P.J. Cherian, K. Radhakrishnan R. Madhavan Nayar Centre for Comprehensive Epilepsy
Care, Sree Chitra Tirunal Institute of Medical Sciences and Technology, Trivandrum
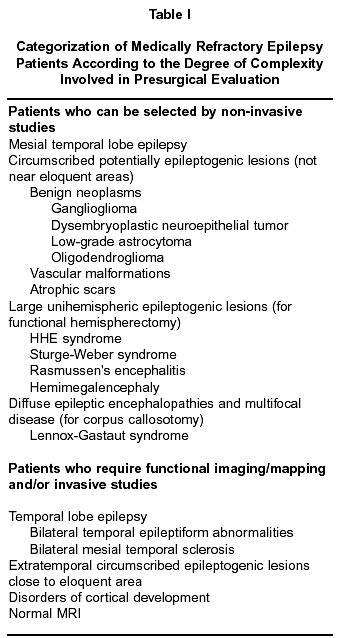
- 695011, Kerala, India. Code Number: ni02005 Summary In order to become cost-effective, epilepsy surgery centers in developing countries will have to achieve excellent results by selecting candidates destined to have a seizure-free outcome using locally available limited technology and expertise, without compromising on patient safety. Our experience illustrates that this goal can be accomplished by selecting patients, whose epileptogenic zone can be unquestionably established, based on history, magnetic resonance imaging, and interictal and ictal scalp electroencephalogram findings. Patients with mesial temporal lobe epilepsy, and those with circumscribed potentially epileptogenic lesions belong to this category. A stepwise approach by reserving more difficult to treat patients to later date as experience develops, or by referring them to a better-equipped center, will help each center to understand its capabilities and limitations and to move forward. It would be essential to work with and educate the local public and professionals, if the epilepsy surgery program in a developing region were to have a lasting impact, It is encouraging to note that, despite major challenges, in the last one-decade, several epilepsy centers in the developing world have not only successfully implemented epilepsy surgery programs, but also have produced results comparable to that from developed countries at a fractional cost. Key words : Developing country, Epilepsy, Presurgical evaluation, Surgery, Temporal lobe epilepsy. Introduction Epilepsy is a major health problem both in developed and developing countries. At any time and in any place, at least 5 out of 1000 population have active epilepsy, and to this burden, new patients will be added every year at a rate of about 50 per 100,000.1,2 Although a majority of patients with newly diagnosed epilepsy will eventually achieve remission, nearly one in five of them continue to exhibit chronic recurrent seizures despite optimal treatment with antiepileptic drugs (AEDs).3 Surgical treatment is an option for selected patients with medically refractory epilepsy, as many as one quarter to one half of them are potential surgery candidates. 4 Epilepsy surgery was considered, till recently, an expensive high technology therapy restricted to the developed world. The recent recognition that a majority of patients with medically refractory partial seizures have surgically remediable lesional syndromes, that can be identified by relatively simple noninvasive studies, has resulted in the evolution of epilepsy surgery programs in developing countries with results comparable to that of developed countries.5 A recent survey revealed that, in 26 of 142 (18.3%) developing nations, at least one center regularly conducted epilepsy surgery.6 In India, the number of epilepsy surgeries reported in the past 5 years is more than thrice the total number of epilepsy surgeries performed in the previous 50 years.7-9 From March 1995 through February 2002, we undertook 394 epilepsy surgeries, 370 of them were anterior temporal lobectomy with amygdalo-hippocampectomy (ATL) for refractory temporal lobe epilepsy (TLE). Among our 213 patients, who have completed 2 years or more of post-ATL follow-up, 166 (77.9%) were practically seizure-free. The success of epilepsy surgery depends upon the early identification of potential surgical candidates, and selecting from them, ideal candidates destined to have a postoperative seizure-free outcome.4,5 Therefore, two basic requirements must be fulfilled before epilepsy surgery program can be introduced in any geographical region: existence of a level of medical infrastructure to identify epilepsy patients with medical refractoriness, and a comprehensive epilepsy care organization where such patients can be subjected to a multidisciplinary evaluation to decide about surgical candidacy. Since epilepsy surgery centers in developing countries will lack the full range of state-of-the-art technologies usually available in centers in the developed world to perform presurgical evaluation and surgery, the success of epilepsy surgery program in a developing country set-up will depend upon the ability to select ideal surgical candidates using locally available technology and expertise without jeopardizing patient safety. Based on our experience, we wish to enlist the difficulties encountered in implementing and sustaining epilepsy surgery programs in a developing country set-up, and elaborate on how to overcome these difficulties. Identification and Ascertainment of Prospective Surgical Candidates Surgical treatment of epilepsy should not be considered as the last resort after all combinations of AEDs have been tried. The natural history studies of epilepsy have shown that most of the patients who are destined to achieve satisfactory seizure control will do so within two years of the onset of epilepsy.3 Continuing frequent seizures during childhood, adolescence and early adult life can produce devastating psychosocial, educational and occupational consequences. Once lifestyle gets fixed, surgical treatment undertaken to successfully terminate the seizures may have little impact on the quality of life of the individual.10 Because of these reasons, in developed countries, more emphasis is recently being placed on early identification of medically refractory epilepsy and prompt referral for surgical treatment.11 If after two years of appropriate trials with AEDs, the patient continues to have frequent disabling seizures, referral to a comprehensive epilepsy care facility should not be delayed. Some level of basic medical infrastructure is necessary to identify patients with chronic epilepsy early and to ensure that proper AED treatment has been tried. There are only about 500 neurologists for the 5 million persons with epilepsy in India. While 70% of the people with epilepsy in India reside in rural areas, almost all the neurologists practice in urban areas.12 A majority of patients with epilepsy in India and other developing countries are therefore treated and followed-up by primary and secondary care physicians, who have little knowledge about the recent trends in the management of epilepsies. To many of them, epilepsy is still an incurable chronic disorder. Epilepsy clinics in a developing country setup have to cater to a large number of patients with very limited skilled personnel. Overcrowding with patients and the consequent overburdening of the service providers, make time available for clinical assessment of individual patients very limited. A frequent difficulty encountered in identifying medical refractoriness among patients with chronic epilepsy in developing countries is that, although many drugs have been used, none were given for sufficiently long periods and in adequate dosages, either alone or in proper combinations.13 Additionally, in some geographic regions, local superstitions and customs would prevent patients from seeking medical and surgical treatment. Even in developing regions with high level of literacy and health awareness such as Kerala, myths and misconceptions about epilepsy and negative attitudes towards persons with epilepsy are widely prevalent.14 These factors contribute to considerable delay in the identification of prospective surgical candidates. If the care of persons with epilepsy in India has to improve at the community level, undergraduate medical curriculum should have more emphasis on this common disorder, and the primary and secondary care physicians need to be regularly updated about the recent advances in the management of epilepsies through continuing educational programs. At the tertiary referral center level, having a weekly or fortnightly subspeciality clinic dedicated for the assessment of difficult to control epilepsy patients will facilitate the ascertainment of prospective surgical candidates. Public education ought to be undertaken through all locally available means such as attractive posters, pamphlets, street plays, television and radio programs, and articles in lay press highlighting the medical aspects of epilepsy and its therapeutic potential, including the surgical option. The efforts being undertaken nowadays by some of the local chapters of the Indian Epilepsy Association and non governmental organizations (NGOs) to improve public awareness about various aspects of epilepsy are commendable. Selection of Ideal Surgical Candidates Patients referred with the diagnosis of refractory epilepsy require a systematic and comprehensive diagnostic and therapeutic evaluation. The objectives of presurgical evaluation are to establish the diagnosis of epileptic seizures and to exclude non epileptic behavioral events, to delineate the lesion responsible for the seizures, to select ideal surgical candidates with optimal electro-clinical-radiological correlation, and to ensure that surgery will not result in disabling neurocognitive deficits.4,5 A comprehensive epilepsy care set-up attached to a tertiary referral medical center with infrastructure, technology and personnel to undertake presurgical evaluation, selection of ideal candidates, surgical treatment and follow-up is necessary to run a successful epilepsy surgery program.5 Technology Evidently, epilepsy surgery centers in developing countries will lack the full range of state-of-the-art technologies usually available in centers in the developed world to perform presurgical evaluation such as positron emission tomography (PET), single photon emission computed tomography (SPECT), functional magnetic resonance imaging (fMRI) and magnetoencephalography.15 The two basic technological requirements that are mandatory for presurgical assessment are a high resolution (1.5T) MRI and video-EEG telemetry. The MRI is the best tool available to define surgically remediable lesions responsible for refractory seizures such as medial temporal sclerosis, cortical developmental and vascular malformations, low-grade neoplasms, and focal atrophic lesions.16 The MRI protocol used for structural imaging should include T1WI in axial and sagittal planes, T2W and proton density sequences in axial and coronal planes, with 5 mm thickness and zero spacing, T1W 3D SPGR images in coronal plane with 1.5 mm slice thickness, and FLAIR sequences, if indicated.16 A majority of the MRIs done outside the comprehensive epilepsy care centers do not conform to these specifications. Repeating the MRI will add to the financial hardship of the patient. In developing countries, one has to utilize the available MRI facilities in a systematic and cost-effective manner to obtain the optimum results. A dedicated neuroradiologist interested and experienced in imaging in epilepsy will bring more dividends than expensive software meant for volume acquisition. The long-term video-EEG monitoring is the most definitive method for differentiation of epileptic seizures from non epileptic events, classification of seizure types, and localization of seizure onset.17 The investment in equipment and the time for monitoring makes this procedure expensive and labor intensive. Furthermore, in a developing country set-up, in the absence of readily available technical support, maintenance and repair of this equipment is difficult and expensive. Setting up the unit at or close to the epilepsy ward can obviate the need for additional personnel to staff the facility. We have shown that by carefully selecting the patients for monitoring and individualizing the objective of the recording, ictal video-EEG monitoring can be used in a cost-effective manner.17 Although we do not routinely use sphenoidal electrodes during long-term video-EEG monitoring, we have found them useful in patients whose initial scalp recorded ictal EEG pattern is poorly visualized or contaminated by movement artifacts.18 The value of intracarotid amobarbital test (Wada test) in the presurgical evaluation of patients with TLE is uncertain.19 The Wada test can be restricted to those patients in whom dominant temporal lobe resection is planned and in whom neuropsychological testing has revealed bilateral or discordant memory dysfunction. The role of intraoperative electrocorticography in predicting the outcome of patients undergoing standard ATL is disputed,20 but is useful when a selective amygdalo-hippocampectomy is planned. Such strategies can prevent unnecessary escalation of the cost of temporal lobe epilepsy surgery. Personnel Epilepsy surgery cannot be performed occasionally on an isolated basis, but must be an uninterrupted welldefined program that utilizes a systematic approach with established criteria for patient selection, surgery, and follow-up. The decision making for epilepsy surgery needs a multidisciplinary approach in which different investigators work in conjunction to create an integrated picture of epileptogenesis.4,5 The minimum personnel required to accomplish these objectives are a neurologist with extensive experience in clinical epileptology and EEG, a neurosurgeon with expertise in epilepsy surgery, a dedicated EEG monitoring technologist, and a clinical coordinator to manage patient scheduling and maintain a database. Additional persons required on a part-time basis are a neuroradiologist, a neuropsychologist, a psychiatrist, a medico-social worker and a biomedical engineer. Such a team approach is not easy to organize and maintain in a developing country set-up, where medicine is still largely practiced on an individual basis. Patient Selection The success of epilepsy surgery program in a developing country set-up will depend upon the ability of the team to select, through a patient management conference, ideal surgical candidates in whom the epiletogenic zone can be unequivocally established using locally available technology and expertise without compromising patient safety. Knowing when not to operate because of the need for further studies is as important as selecting which patients may benefit from surgery with the limited facilities available, which needs considerable experience and a team approach. Patients with medically refractory epilepsy belong to different categories depending upon the degree of complexity involved in presurgical evaluation and the postoperative seizure outcome (Table I). The prototype of a surgically remediable syndrome is mesial TLE (MTLE), the type of TLE associated with hippocampal sclerosis, which constitutes more than half of those patients with medically refractory epilepsy worldwide.21 Non-invasive evaluation utilizing history, MRI, scalp video-EEG, and neuropsychological findings can identify patients with MTLE and those with other circumscribed, potentially epileptogenic lesions, 70% to 90% of whom become seizure-free following resective surgery.4,8,9,22,23 Selected MTLE patients with consistent unilateral temporal interictal epiletiform abnormalities may not even require ictal video-EEG recordings.24 Patients with large epileptogenic lesions involving primarily one hemisphere, and those with diffuse epileptic encephalopathies and multifocal disease can be selected for functional hemispherectomy25 and corpus callosotomy,26 respectively, based on noninvasive data. Patients with extratemporal partial seizures, disorders of cortical development, and those with normal MRI will require extensive, sometimes repetitive studies with SPECT and intracranial electrode placement, which enormously escalate the cost of presurgical evaluation.27 Even with these expensive evaluations, in the later group of patients, the postoperative outcome is often not favorable.4,27 Surgical Treatment Gap The population of the developing world is 5 times the size of the developed world, but has at its disposal only 5% of the global per capita gross domestic product (GDP).6 Developing countries are home to nearly 90% of the people with epilepsy worldwide, but are the ones least prepared to provide optimal care for them.28 India, with over one billion inhabitants, may have approximately one million persons with medically refractory epilepsy; among them as many as one quarter to one half are potential surgical candidates. However, no more than 100 epilepsy surgeries are currently being performed per year in India.5 Thus only a miniscule of potential surgical candidates in India and other developing countries ever get a chance to undergo presurgical evaluation. The lack of availability and affordability has resulted in an enormous gap in developing countries between number of patients who could be benefited from epilepsy surgery and those who actually receive this treatment, which can only be minimized by developing more centers in the country, where epilepsy surgery can be undertaken. Although the total direct cost of presurgical evaluation and surgery in developing countries amounts to a small fraction of the cost incurred in the industrialized world,9,22 this expenditure is beyond the reach of the majority. The out of pocket payment for ATL (including presurgical evaluation) in Indian set-up is Rs. 50,000. The direct total cost for caring a TLE patient from age 26 to 60 years has been calculated to be Rs. 200,000.9 Even with new AEDs, complete seizure freedom is less than 10% for TLE patients.29 There is over 70% chance that the patient will be seizure-free after ATL, and a 30% chance that the patient is completely off AEDs within 2 years after ATL.9 A recent randomized, controlled trial confirmed that the seizure outcome is far superior in surgically treated refractory TLE patients when compared to those continued on AED treatment.30 A seizure-free person could be better employed, achieves an improved quality of life and often becomes a productive member of the society.31,32 Therefore, surgical treatment of refractory TLE is definitely a better cost-effective option than continued medical treatment. National epilepsy organizations and epilepsy centers in developing countries could effectively use these statistics to obtain governmental subsidies and non-governmental financial supports for implementing and sustaining epilepsy surgery programs. Acknowledgement We wish to thank our colleagues in the R. Madhavan Nayar Center for Comprehensive Epilepsy Care for their contributions. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02005t1.jpg] |
| |||||||||

{kind=link}