 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 33-36 The Lateralizing Significance of Version of Head and Dystonic Limb Posturing in Epileptic Seizures G. Shukla, M. Bhatia, S.B. Gaekwad*, V.P. Singh,** S. Jain, M.C. Maheshwari Departments of Neurology, Neuroradiology,* Neurosurgery**,
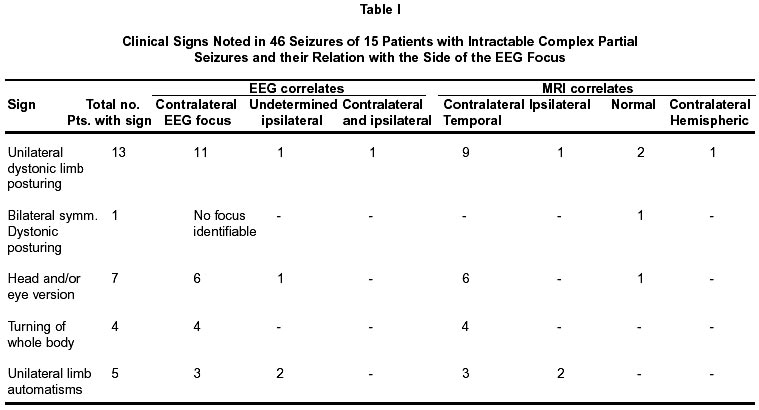
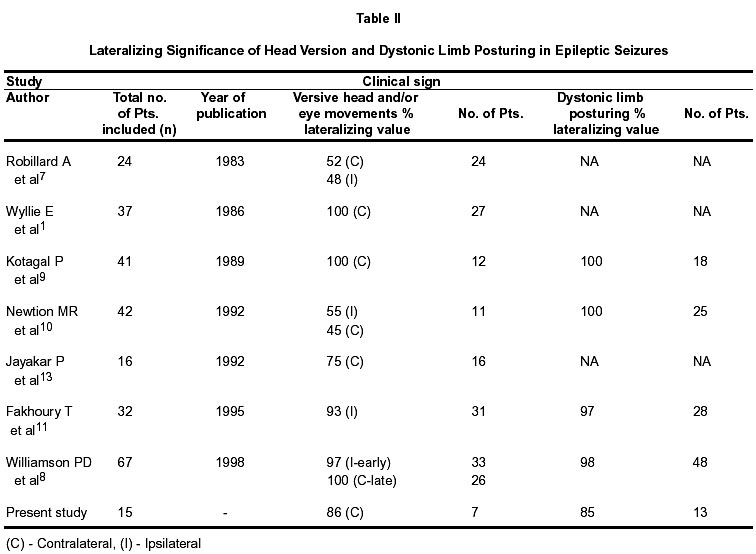
All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110 029, India. Accepted for publication : 30th January, 2001 Code Number: ni02009 Summary Several clinical signs have been described for lateralization and localization of seizure focus in complex partial seizures; however, the specificity of each of these has been widely debated upon. The present study was done to evaluate 'dystonic unilateral limb posturing' and 'versive head movements' for lateralization and localization of epileptic foci in patients with intractable partial complex seizures, being investigated with long term Video-EEG monitoring. Fifteen patients with 46 seizures, studied with long term Video EEG, had either one or both of these signs. The video recordings of the clinical behaviour were noted and later compared with the corresponding EEG. Unilateral dystonic limb posturing and versive head movements had good lateralising value in complex partial seizures, suggestive of temporal lobe origin, contralateral to the seizure focus, with a specificity of 87.5% and 86% respectively. In addition, turning of the whole body to one side was associated with a contralateral seizure focus in 100% cases. Appendicular automatisms were found to be of no lateralising significance, as they occurred on either side with equal frequency. These motor phenomena should, therefore, be enquired about in detail, during history taking for lateralization or localization of seizure focus. Key words : Lateralising signs, Dystonic posturing, Complex partial seizures. Introduction The value of various clinical signs, such as head and body turning in simple as well as complex partial seizures,1-8 unilateral eye blinking, automatisms, tonic posturing, ictal speech, post ictal dysphasia and facial asymmetry in complex partial seizures1,4,7 has been variably emphasised for localisation and lateralization of an epileptic focus. However, it has also been equally questioned and debated upon.7,9 The aim of the present study was to evaluate 'dystonic posturing' and 'versive head movements' in lateralization and localization of epileptic foci in patients with intractable epilepsy. Materials and Methods Fifteen patients with 46 spontaneous epileptic seizures were selected from the group of patients undergoing long-term VEEG monitoring as work-up for epilepsy surgery, because they had head and/or eye version or had dystonic limb posturing or both. Versive movements were defined as clonic or tonic head and eye deviations, which were unquestionably forced and involuntary, resulting in sustained unnatural positioning of the head and eyes. Contraversive head and eye movements were directed away from the hemisphere of onset; and ipsiversive movements turned towards that hemisphere.1 Unilateral dystonic posturing was defined as forced, unnatural posturing of an arm or leg on one side of the body. This posturing was either in flexion or extension; proximal or distal, or usually with a rotatory component. It could be easily distinguished from tonic posturing, in which there is only extension or flexion without accompanying rotation or assumption of unnatural postures.9 Video EEG monitoring was done with surface electrodes placed according to the 10-20 system of electrode placement. The EEG data was stored in the hard disk, along with the patient's video on a videocassette in a split screen format. These were reviewed by neurologists (GS and MB). The sides of dystonic posturing, versive movements, and automatisms were noted in all and their ictal EEG correlates determined. MRI was done on all the patients and the abnormalities recorded. The dystonic posturing and head version were correlated with the ictal EEG and MRI. Results Fifteen patients with 46 seizures were selected for this study. The age range was between 10 and 45 years (mean 24 years). Five patients were females, while ten were males. Dystonic limb posturing was seen in 14 patients; 13 had unilateral posturing and 1 patient had bilateral simultaneous and symmetrical posturing. Among these 14 cases, 7 patients (20 seizures) had isolated dystonic posturing while the other 7 patients (23 seizures) had accompanying head and/or eye version as well. An interesting sign, i.e. turning of the whole body towards one side, was seen in a total of 4 patients. This was the only localising sign in one patient (3 seizures), while 3 patients (10 seizures) had this sign in addition to same sided dystonic limb posturing. None of the patients had isolated head or eye versive movements. Automatism was observed in 10 patients. It was bilateral in 5 patients, occurring simultaneously on both sides in 2 patients. In 3 patients, it occurred on the side opposite to that of the dystonic posturing at the onset; but later occurred in the same limb as the posturing. In the remaining 5 patients, who had unilateral automatism, 3 had automatism in the limb opposite to the side of dystonic posturing; in the other 2 patients, it involved the side same as that of dystonic posturing. Two patients also had simultaneous facial automatism. Table I demonstrates these clinical findings in correlation with the EEG foci in all patients. EEG and MRI Correlates EEG focus was contralateral in 11 out of the 13 patients (40 seizures) with unilateral dystonic limb posturing. MRI revealed a lesion in the temporal region on the same side as the EEG focus in 9 patients; one patient had diffuse hemispheric involvement with multiple infarcts and atrophy on the same side as the EEG focus, while the MRI was normal in one patient. In the 12th patient, who had 3 seizures, EEG focus was contralateral to dystonic posturing in one seizure, and ipsilateral to the focus in the other two seizures. The MRI of this patient was also normal. The 13th patient had left upper limb dystonic posturing in all her 3 seizures but the EEG focus could not be determined due to very rapid generalisation at ictal onset. The MRI revealed a welldemarcated lesion in temporal lobe, ipsilateral to that of the dystonic posturing. Seven out of the 13 patients (23 seizures) had head version in addition to dystonic limb posturing. Six demonstrated an EEG focus opposite to the side of head turning. The 7th patient in this group is the same as the 12th patient described above, who had the EEG focus ipsilateral to the head version in all seizures. Four patients with turning of the whole body towards one side, had most consistently a contralateral EEG focus. MRI revealed a lesion on the side of the focus in all the four cases. Automatisms seemed to have no localising significance. Five patients had bilateral automatisms; 4 of these had a right-sided focus and 1 had a leftsided focus. Among the 5 patients with unilateral automatisms, 3 had a contralateral EEG focus and 2 had an ipsilateral focus. Discussion Dystonic limb posturing, head version and turning of the whole body to one side were the clinical signs of good lateralising value, in this study, in patients of complex partial seizures. The findings regarding limb posturing are in congruence with those of several others. Kotagal et al pioneered in describing dystonic limb posturing as a reliable lateralising sign,9 in a study of 41 seizures. 18 patients with 41 seizures, had unilateral dystonic limb posturing, contralateral to the electroencephalographically proven epileptogenic focus. This was further confirmed by good results of epilepsy surgery targeted at the focus. Newton et al10 described clinical features of 40 out of 42 patients, in whom clinical, EEG and neuroimaging data indicated a temporal lobe origin of seizures. Twenty-five patients, among these, had dystonic upper limb posturing as a valuable lateralizing sign. In all the cases, the side of maximum dystonia was contralateral to the side of the epileptic focus. In this study, ictal- SPECT studies were also conducted, which showed a significant activation of basal ganglia in patients having dystonic limb posturing. Fakhoury and Abou- Khalil11 described similar results in their series and recorded that 97% cases had dystonic posturing contralateral to the seizure focus. In the present study, 87.5% had dystonic posturing contralateral to seizure focus. Unlike dystonia, head and eye version is still controversial as a reliable lateralising or localising sign. One reason for this debate, is the variation in the definitions of head version. Robillard et al7 and Ochs et al2 studied this sign and found it of no lateralizing value. They, however, did not use the strict definition of head version.1 Wyllie et al1 found versive head and eyes movements in 27 patients out of a total of 37 in their study and these movements occurred contralateral to the EEG focus in all patients. The recent concept proposed by Fakhoury and Abou- Khalil11 and later by Williamson et al8 about early ipsilateral, and late contralateral version was, however, not observed by us. Various studies stressing significance of the discussed clinical signs in lateralization of epileptic foci are compared in Table II. It is to be re-emphasised that turning of the whole body, not very much stressed upon previously, has also been observed by us as a highly reliable lateralizing sign, having occurred consistently contralateral to the EEG focus. Conclusion Dystonic limb posturing, head version and turning of the whole body are clinical signs with good lateralizing value in complex partial seizures, where site of onset is difficult to determine. This stresses the need to ask for these phenomena when evaluating patients with complex partial seizures in order to determine the site of seizure origin. The EEG focus is contralateral to the abnormal posturing. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02009t2.jpg] [ni02009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}