 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 37-40 Prognostic Factors Influencing the Outcome of Thalamic Glioma S. Pathy, S. Jayalakshmi, S. Chander, R. Singh,* P.K. Julka, G.K. Rath Departments
of Radiation Oncology and Biostatistics*, All India Institute of Medical Sciences,
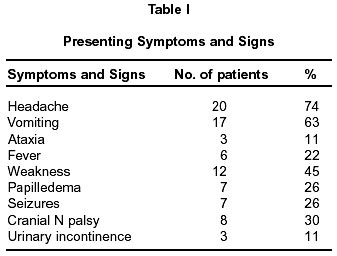
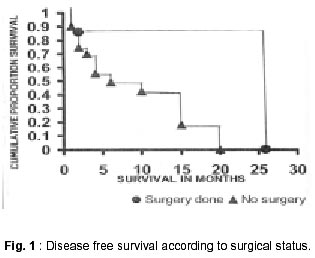
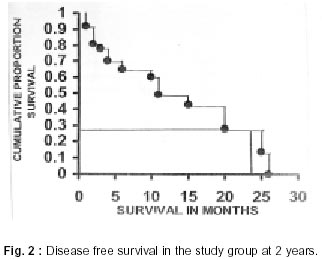
Ansari Nagar, New Delhi - 110 029, India. Accepted for publication : 8th March, 2001. Code Number: ni02010 Summary Retrospective analysis of 27 patients of thalamic glioma including adults and children treated over a period of 7 years from 1991-1997 was done. The study group included 19 males and 8 females; 9 patients were less than 15 years and 18 patients more than 15 years of age at the time of diagnosis. The commonest symptoms were headache and vomiting. 12 patients underwent VP shunt as an initial procedure and 7 underwent total or partial surgical resection. Confirmed histopathological examination was possible in 16 patients; while 12 had low grade astrocytoma, 4 cases had high grade histology. All patients were treated with radiotherapy to a total dose of 50-60 Gy in 25-30 fractions. Median follow up was 9.63 months. The disease free survival in these patients was 28% at 2 years. Prognostic factors which included age, sex, duration of symptoms, surgical procedures, histology and radiotherapy dose were evaluated for significance. A subtotal resection conferred a better prognosis. Key words : Thalamus, Radiotherapy, Brain neoplasm. Introduction Thalamic and brain stem tumors constitute 10-15% of primary intracranial gliomas of childhood,1,2 with a dominant age being 4-14 years. Adult thalamic and brain stem tumors constitute 35%.3 Due to their critical location, thalamic tumors often require treatment without biopsy confirmation. However, autopsy results and more recently stereotactic biopsy have revealed that the majority of the tumors are glial neoplasms.4 The treatment of intrinsic brain stem and thalamic tumors often results in poor outcome.5-7 Total surgical resections are generally less feasible because of the resulting neurological deficits. Standard radiation therapy in doses of 50 to 60 Gy may result in median survival of 1 year.8 Radiation therapy continues to be the primary modality of treatment for children with brainstem and thalamic tumors. The survival in pediatric age group varies from 10-70%, whereas in adults it ranges from 5- 50%.9 This study includes the analysis of 27 patients of thalamic glioma in both adults and children, treated over a 7 years period from 1991-1997. Material and Methods This is a retrospective analysis of 27 patients of thalamic glioma treated in the department of Radiation Oncology, All India Institute of Medical Sciences, from Jan 1991 to Dec 1997. The disease profile, presenting symptoms, signs and treatment modalities are detailed in the study. Initial CT scans and MRI scans were reviewed in detail. All patients were treated with radiotherapy. Survival data was calculated from beginning of irradiation. The statistical significance and differences in survival between patient groups and various prognostic factors were analyzed. The patient group consisted of 19 males and 8 females. Nine patients were less than 15 years and 18 were more than 15 years of age, at the time of initial diagnosis. The common symptoms were headache (20 cases) and vomiting (17 cases). The mean duration of symptoms was 9.59 months. Table I shows the presenting symptoms and signs in detail. Duration of symptoms was less than 6 months in 20 cases. Seven patients had a duration of more than 6 months. 12 patients underwent ventriculo-peritoneal shunt prior to radiotherapy. 7 patients underwent either total or partial surgical resection. Those patients who could not be biopsied because of the location of the lesion were presumed to have primary glioma based on radiological findings. Histopathological diagnosis after stereotactic biopsy was available in 16 patients. Twelve patients had low grade astrocytoma while 4 had high grade histology. All patients were treated with radiotherapy to the tumor. Radiotherapy was delivered using Co60 megavoltage equipment. The treatment volume was planned with margin of 2-3 cm outside the tumor and peritumoral edema. Parallel opposed portals were most commonly used. A total dose of 50-60 Gy in 25- 30 fractions was planned over a period of 5-6 weeks. Nineteen patients received dose of more than 50 Gy, while remaining 8 patients received less than 50 Gy. The dose of glucocorticoids was adjusted as necessary to improve the level of neurological function, to reduce headache, vomiting and was maintained at the lowest dose needed to control these manifestations. Anticonvulsants and antiemetics were used wherever indicated. Patients were evaluated neurologically and by radiological studies to see the residual or recurrent tumor. The median followup was 9.63 months. 8 patients were lost to follow up. Results The median survival time was determined according to age and sex. Significance was determined at p < 0.05.10 According to age, the median survival in 9 children was 9.5 months (95% confidence limit - 4) and in 18 adults was 8.9 months (95% confidence interval 3-15) the difference was not statistically significant (p = 0.1295). According to sex, the median survival in 19 males was 7.29 months (95% Cl - 3.0) and in 8 females was 15 months (95% Cl - 4). The difference was not significant (p = 0.7339). 20 patients with a shorter duration of symptoms (less than 6 months) (95% confidence interval 2-15) had median survival of 4 months and 7 patients with symptoms for more than 6 months had median survival 14 months (95% Cl - 11). The difference was not statistically significant (p = 0.07). 12 patients with a VP shunt had median survival of 4 months (95% Cl - 3) which was not significantly different from median survival of 15 patients without VP shunt (95% Cl - 10) p = 0.1323. Seven patients who underwent surgical procedure involving total/subtotal resection had median survival of 12 months (95% Cl not calculable) as against median survival of 5.82 months in 20 patients who did not undergo surgery (95% confidence interval 3-15) and the difference between the two was statistically significant (p = 0.0087) (Fig. 1). 8 patients, who received radiotherapy dose of less than 50 Gy, had a median survival of 4 months (95% Cl - 1) and 19 patients who received radiotherapy dose of more than 50 Gy, had a median survival of 11 months (95% Cl - 4) and the difference between the two was not statistically significant (p = 0.51). Discussion The symptoms and signs at presentation in thalamic tumors are related to the size and extent of the tumor and the presence of increased intracranial tension. The presenting symptoms and signs in this study are similar to those outlined in the literature.9,11 Ten patients presented with a longer symptomatology (more than 6 months). This is similar to the report of 136 patients by Grigsby et al, where only 17.8% of the patients presented with symptoms which persisted for more than 6 months.11 In the present series, there were 18 adults and 9 children. Lee, in his series of 41 patients, observed that 60% of the thalamic tumors occurred under 16 years of age.12 In the present series, a histological diagnosis was possible in 16 patients. Increased use of steroids and stereotactic biopsy techniques have increased the probability of obtaining tissue for diagnosis and in reducing their attendant risk.4 The information gained from biopsy will result in tailoring of treatment, meaningful modifications of treatment, designing experimental treatment approaches and in determining prognosis. In the present series, 3 of the 16 biopsied tumors were glioblastoma multiforme (GBM). Ryoo et al, in their analysis of the histological patterns of the biopsies peformed in 172 of 463 patients in various series, observed that GBM has been reported in 71 patients. It is significant to note here that the above included thalamic and brain stem tumors.13 Tumor histology has been reported to affect survival in both pediatric and adult patients.6,11,14 A histological diagnosis of GBM did not confer a poor prognosis in the present series. This could be due to the small number of GBM in the histologically proven tumors in this series, which did not contribute to statistical significance. Patients who underwent total or subtotal resection in our series had a significantly prolonged median survival in comparison to those who did not undergo surgery (p = 0.0087). Grigsby et al in their analysis of thalamic and brain stem gliomas have highlighted the fact that the patients undergoing subtotal resection had a relatively good prognosis.11 Such a finding has been acknowledged by Freeman and Swissa.6, We did not find any response to radiotherapy. Eifel et al in their report of thalamic gliomas also did not find any response with radiotherapy using 49-56 Gy.9 The radiation doses used in those tumors have ranged from 45-60 Gy in conventional fractionation.9,11,15 The last two decades have seen the emergence of hyperfractionation and an effort to increase the total radiotherapy dose to 76 Gy - 78 Gy in order to achieve better local control. Prados et al reported a median survival of 12.7 months by administering radiotherapy, in hyperfractionation schedule to a total dose of 76 Gy.8 Halperine assessed the size of radiation field employed on survival and patterns of treatment failure. Since the majority of the treatment failures were in the initial tumor volume, no advantage in local control accrued from whole brain fields. Thus radiation therapy fields encompassing CT definition of tumor, surrounded by an adequate margin is sufficient to prevent a geographic miss.15 The complication of treatment and quality of survival have been assessed by Eifel. The majority of surviving children seem to have good functional results and relatively normal life.9 Grigsby et al, in assessing the neurological function and sequelae following radiation therapy, found that in a follow up ranging from 3-22 years, 57.6% of 33 surviving patients had normal neurological function of minimal neurological deficits.11 Treatment related sequelae in long term survivors of hyperfractionation radiation therapy have been evaluated by Freeman et al and enumerated as schooling difficulties, seizure disorder, hearing loss, decreased growth hormone secretion and changes in imaging studies viz. leukoencephalopathy, diffuse micro hemmorhages and dystrophic calcification.16 Few authors have detailed the prognosis in thalamic gliomas and have attempted to relate it to treatment factors. Jentzsch et al made an effort to correlate the tumor volume response to radiation therapy to the prognosis.17 They found a post treatment increase in tumor size in 4 patients with low grade gliomas which did not correlate with poor prognosis. Three high grade tumors regressed promptly after radiotherapy and all recurred. In contrast, poor prognosis in adult patients with GBM, that substantially increased in size during treatment has been reported, whereas there was no impact on prognosis in adult patient with grade III glioma that increased to a smaller degree.12 The disease free survival at 2 years, in this series was 28%. The overall 5 year survival has been reported as around 73%.11,15 Grigsby et al elicited that the overall 5 year survival in thalamic tumors in pediatric patients was 59.5% and was significantly better than in adults (20.9%) (p = 0.006). Survival was favourably correlated with low grade histology and subtotal surgical resection in the same series. 11 References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02010t1.jpg] [ni02010f1.jpg] [ni02010f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}