 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 41-44 CSF Beta-1 Globulin - A Potential Marker in Differentiating Multiple Sclerosis and Acute Disseminated Encephalomyelitis : A Preliminary Study B. Chopra, R. Abraham, A. Abraham* Departments of Biochemistry and Neurology*,
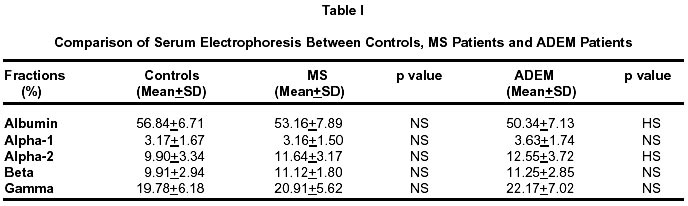
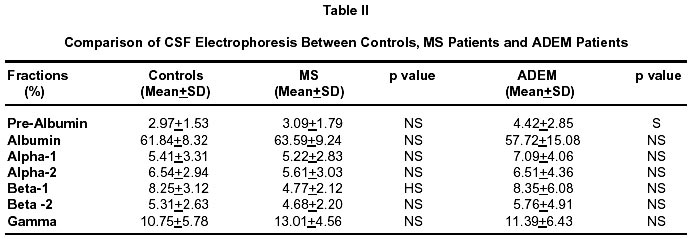
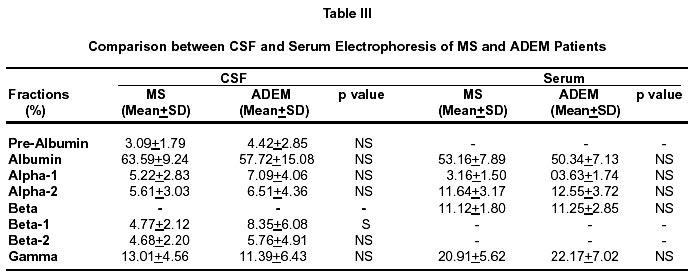
Christian Medical College and Hospital, Ludhiana, Punjab, India. Accepted for publication : 21st October, 2000. Code Number: ni02011 Summary The exact diagnosis of demyelinating diseases is an enigma even in the best neurological centres. In the present study, the potential role of differential CSF proteins has been critically evaluated in differentiating multiple sclerosis (MS) and acute disseminated encephalomyelitis (ADEM). Cellulose acetate electrophoresis was carried out on CSF and serum samples of 14 MS patients, 23 ADEM patients and 30 controls. There was no statistically significant difference between serum electrophoresis of controls and MS patients. However, in case of CSF electrophoresis there was a statistically significant decrease in beta-1 fraction in 92.2% of MS patients (p=0.01). A comparison between serum electrophoresis of controls and ADEM patients indicated a statistically significant decrease in serum albumin in 87% patients and an increase of alpha-2 globulin in 73.9%. There was no statistically significant difference between CSF electrophoresis of controls and ADEM patients except for the prealbumin fraction which was raised in 60.9% of patients. No statistically significant difference was seen between the serum electrophoresis of ADEM and MS patients. However, on comparing CSF electrophoresis, it was seen that beta-1 fraction was significantly higher in ADEM patients (p<0.05). The predictive value of beta- 1 fraction in differentiating MS and ADEM was then evaluated. The negative predictive value was 100% indicating that all samples with a beta-1 fraction of >6.5% cannot be diagnosed as MS. The significant decrease in beta-1 fraction in MS patients may prove to be an early indicator in differentiating between MS and ADEM patients. Key words : Acute disseminated encephalomyelitis, CSF electrophoresis, Multiple sclerosis, Protein fractions, Serum. Introduction The exact biochemical diagnosis of demyelinating diseases is a challenge even in the best neurological centres. Kabat et al1 were the first to perform electrophoresis of CSF in 1942 and reported increased gamma globulins in multiple sclerosis (MS). In recent years, the electrophoresis of CSF and serum has been carried out extensively.2-6 An increase in gamma globulins has been recognized as an important factor in the diagnosis of demyelinating disorders. In India, Prabhakar et al,7 in a preliminary study in 1990, analyzed immunoglobulins in the CSF and serum of a small number of patients with demyelinating diseases, subacute sclerosing panencephalitis, brain tumors and meningitis. The present study was undertaken to understand the role of total and differential CSF and serum proteins in differentiating multiple sclerosis (MS) from acute disseminated encephalomyelitis (ADEM). Material and Methods CSF and serum samples were collected from 30 controls undergoing surgical procedures under spinal anesthesia with no history of any neurological disorder. The diagnosis was based on clincial and CT/MRI criteria. 14 cases of MS and 23 cases of ADEM patients diagnosed by a neurologist were enrolled in the study. Cellulose acetate (Sartorius AG - 37070 Goettingen, Germany) electrophoresis8 was carried out on all CSF and serum samples. Barbitone buffer was prepared by dissolving 10.3g of sodium barbitone and 1.8g of diethyl barbituric acid in double distilled water and the final volume was made upto one litre. The pH was adjusted to 8.6 by a pH meter. Ponceau S stain was prepared by dissolving 500mg of Ponceau S in 3% trichloroacetic acid. Barbitone buffer was filled in the Gelman electrophoresis tank. The cellulose acetate strips were labelled, then wet in the buffer and blotted with a filter paper to remove excess buffer. The CSF samples were applied on the strips with a twin wire applicator. The CSF samples were not concentrated but each sample was applied thrice on the same strip on the same spot with the applicator. The strips were then placed in the electrophoresis tank and a constant voltage of 250V and a current of 1.5mA/strip was applied for one hour. Then the strips were stained with Ponceau S for 10 minutes. The excess stain was removed by washing the strips in acetic acid (50ml/l in water). The strips were then scanned on a Beckman (CDS-200) densitometer at 520 nm. The percentages of the various proteins present in the samples were calculated from the area under the curve in the densitometer scan. Electrophoresis of serum samples was carried out in a similar manner. The data was analyzed statistically and 't' test was used to determine significance. Results Comparison between serum electrophoresis of controls and MS patients showed no statistically significant difference. Table I shows a comparison between serum electrophoresis of controls and ADEM patients. Serum albumin showed a highly significant (p=0.01) fall in 87% of ADEM patients. Mean value of alpha-2 was higher in 73.9% of ADEM patients and this was statistically highly significant (p = 0.01). A comparison between CSF electrophoresis of controls and MS patients (Table II) showed that beta- 1 fraction was decreased in 92.2% of MS patients, which was highly significant (p = 0.01). Comparison between CSF electrophoresis of controls and ADEM patients showed a statistically significant (p=0.05) rise of pre albumin fraction in ADEM patients (Table II). Comparison between serum and CSF electrophoresis of MS and ADEM patients shows that beta-1 fraction was significantly higher in CSF of ADEM patients. The remaining fractions did not show any statistically significant difference (Table III). Predictive value of beta-1 fraction in differentiating MS and ADEM was analyses. At a cut off level of 6.5% its negative predictive value was 100%. Discussion Electrophoresis of serum and CSF were performed simultaneously, as slight damage to the blood CSF barriers may allow serum changes to appear in CSF.9 The cellulose acetate methodology adopted for CSF electrophoresis is one of the standard techniques used in the past. When the same methodology was adopted in the controls and the diseased states, the differences seen on statistical analysis became significant. This is a preliminary study and larger studies shall be undertaken in the future by adopting the latest techniques of electrophoresis. Serum electrophoresis in MS patients was not significantly different from controls indicating that the disease process does not affect serum proteins. Comparison between serum electrophoresis of controls and ADEM patients, however, showed decrease of albumin fraction and increase of alpha-2 fraction in 87% and 73.9% ADEM patients respectively (Table I). No earlier studies are available in the literature where these fractions have been compared between serum of controls and ADEM patients. Beta-1 fraction was found to be significantly lower in 92.9% of MS patients (Table II) on comparing CSF electrophoresis of MS cases and controls. The other fractions did not show any statistically significant difference. Beta-1 globulin or transferrin is an iron binding protein, belonging to the beta globulin group, as differentiated by CSF electrophoresis.10 This protein is identical to the serum transferrin. Beta-2, another transferrin, is also present in the CSF. However, there is some uncertainty regarding its origin. The relative concentration of beta globulins is somewhat higher in normal CSF than in serum. However, no specific correlations with neurological diseases have been established with regard to these proteins.10 There is one report on beta-1 globulins11 where raised levels of transferrin were observed during exacerbation of MS. The authors reported that these may be due to release of the protein as a result of demyelination during an exacerbation or due to increased synthesis within the CNS. There is no other reported work describeing changes of beta-1 globulin in MS. However, this protein was lowered significantly in MS patients in the present study and is at variance with the findings of above study which was carried out more than two decades ago. The results from the present study suggest that the lowered levels may be due to down regulation of transferrin receptors in MS patients. Transferrin is known to come from serum10 and is taken into cells by pinocytosis that involves transferrin receptors. It is suggested that these receptors may have been down regulated over months or years in MS, which is a chronic process, and resulted in lesser amounts of transferrin crossing over to the CSF. It is emphasized that more studies on a larger number of patients will crystallize the importance of the results found in the present study. It has also been observed in the present study that prealbumin fraction was increased in the CSF electrophoresis of ADEM patients when compared with controls (Table II). This observation is significant although no comparable studies on this parameter are available in literature. This factor could prove to be helpful in the diagnosis of ADEM. A comparison was made between CSF and serum electrophoresis of MS and ADEM patients which revealed a 100% negative predictive value of beta-1 fraction at a cut off level of 6.5%, when a diagnosis of MS cannot be made. This needs to be confirmed by widening the sphere of such a study to other demyelinating disorders. Conclusion This study indicates that routine CSF electrophoresis and evaluation of, particularly, the beta-1 fraction has potential clinical significance. The significant decrease in beta-1 fraction in MS could prove to be an early indicator in differentiating between MS and ADEM. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02011t2.jpg] [ni02011t3.jpg] [ni02011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}