 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 63-67 Dexamethasone Therapy for Bacterial Meningitis in Adults : A Double Blind Placebo Control Study D. Gijwani, M.R. Kumhar, V.B. Singh, V.S. Chadda, P.K. Soni, K.C. Nayak, B.K. Gupta Department of Medicine, S.P. Medical College, Bikaner- 334 003,
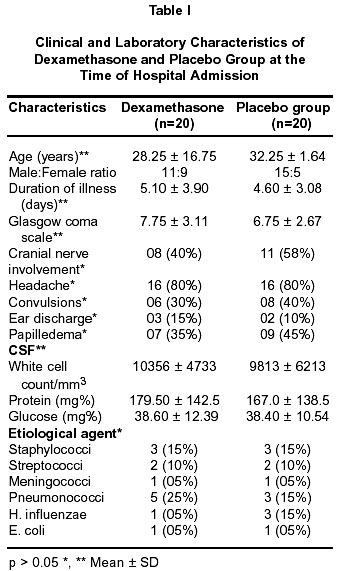
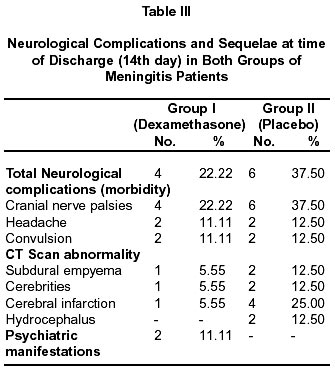
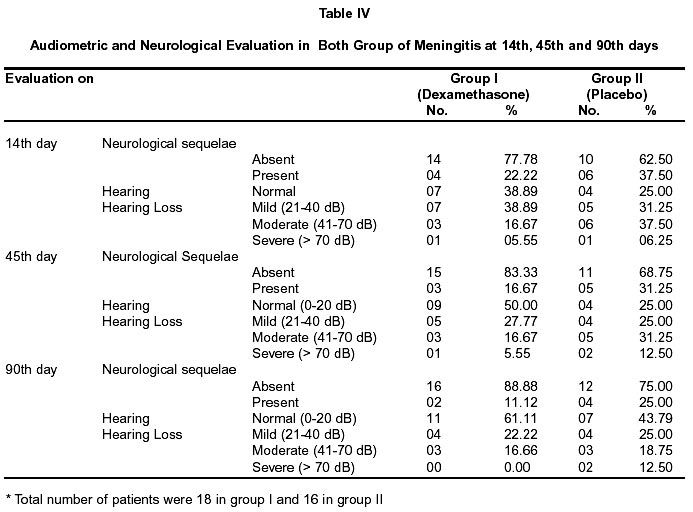
Rajasthan, India. Accepted for publication : 26th May, 2001. Code Number: ni02015 Summary Routine use of steroids in the treatment of bacterial meningitis remains controversial. A prospective placebo controlled double blind study of dexamethasone was carried out in 40 patients (age>10 years) of acute bacterial meningitis. The patients were randomly assigned to receive either placebo (n=20) or dexamethasone (n=20) in addition to injection ceftriaxone 100 mg/kg/day (maximum 4 gm/day) for 14 days. Dexamethasone sodium phosphate was given in dose of 0.6 mg/kg/day in 4 divided doses, for first 4 days of therapy. First dose of dexamethasone was given 15 minutes prior to first dose of ceftriaxone. Baseline demographics, clinical and laboratory features of the two groups were similar. Clinical improvement of signs of meningeal irritation was rapid in dexamethasone group than in the placebo group, but no significant difference was observed regarding resolution of fever, headache and vomiting. Secondary fever (mean+SD 15.00), gastrointestinal tract bleeding (mean+SD 15.00) and psychiatric manifestations (mean+SD 10.00) were more common in dexamethasone group. Neurological complications and hearing loss were more common and severe in placebo group as compared to the dexamethasone group (p<0.05). It is concluded that dexamethasone may be beneficial in some aspects of bacterial meningitis, in adults. A study with a larger number of cases in each group is recommended. Key words : Dexamethasone, Bacterial meningitis, Adults. Introduction Bacterial meningitis continues to be an important cause of morbidity and mortality despite the availability of newer effective antibiotics.1,2 Prospective studies have documented permanent sensorineural hearing loss in approximately 10% of survivors of bacterial meningitis as a whole and 31% of survivors of pneumococcal meningitis.3 In recent years, several investigators have re-examined and reviewed the pathophysiological mechanism operating in meningitis with an aim of improving the outcome. They found that subarachnoid space inflammation and various inflammatory cytokines have a major role in pathophysiology of bacterial meningitis that contributes to morbidity and mortality. Corticosteroid (dexamethasone) as an anti- inflammatory agent has been used to block the secondary release of cytokines and toxic intermediate from brain stem and to stabilize altered vascular permeability.4,5 The role of dexamethasone is controversial in adult bacterial meningitis, though most studies in children support its use.6-8 Dexamethsone has been shown to significantly decrease the case fatality and overall neurological sequelae of bacterial meningitis in both children and adults.9-11 Material and Methods The study was carried out in department of medicine, S.P. Medical College and A.G. Hospitals, Bikaner, from January 1998 to June 1999. Established cases of pyogenic meningitis of more than 10 years of age were included in the study, after obtaining written consent. All the cases had at least one of the following criteria12 : i) turbid or purulent CSF with identification of bacteria on Gram staining or culture of CSF, ii) CSF leukocytosis (>10 to <10,000/cumm) with neutrophils predominance iii) elevated CSF protein above 50 mg/dl and glucose less than 40 mg%. Patients treated with antibiotics before the first dose of dexamethasone, any patients with congenital or acquired abnormality of central nervous system, patients with recurrent meningitis, post traumatic meningitis, diabetes mellitus, hepatic and renal dysfunction were excluded from the study. Treatment Protocol : Equal number of patients were included in both the groups i.e. 20 in dexamethasone group and 20 in the placebo group. Randomization was done by odd and even number of patients. Odd numbered patients was included in the dexamethasone group and the even numbered in the placebo group. Patients were randomly assigned to receive either dexamethasone (Group I) or placebo (Group II) in case control manner. In this study, 2 ml vials were prepared which contained either inactive ingredient (placebo) or 4 mg of dexamethasone sodium phosphate per ml. All vials contained a clear colorless solution and were identical in appearance. Group I patients received dexamethasone phosphate, 0.6 mg/kg/day in 4 divided doses for first 4 days of therapy. First dose of dexamethasone was given at least 15 minutes prior to first dose of ceftriaxone.6,13 The Group II patients received equal volume of normal saline in place of dexamethasone. Both groups received 100mg/kg/day ceftriaxone (maximum 4gm/day) for 14 days.3 The relevant investigations, including detailed biochemistry, microscopic examination, Gram staining of CSF, culture and sensitivity of blood and CSF and CT scan of head were done in every patient. The detailed neurological examination and audiometery were performed at discharge on 14th day and on follow-up at 45th and 90th days for neurological complications and hearing loss. Staff carrying out follow-up audiometery and neurological examination were unaware of treatment assignment. Audiometric threshold were determined at 250, 500, 2000, 4000 and 6000 Hz and results were interpreted by the same audiologist who had performed the test. The degree of hearing impairment was classified as no response (21 to 40 dB), mild (41 to 55 dB), moderate (56 to 70 dB), severe (71 to 90 dB) and profound (> 90 dB).13 A quantitative comparison of severity of complications between both groups were attempted by assigning arbitrary numerical score to different complications.14 The complication score (0-6 mild, 7- 12 moderate and 12-18 severe) was designed to reflect the severity and duration of neurological complications and sequelae to reflect the functional damage resulting from meningitis. Results There was male preponderance with male to female ratio of 1.8:1. The CSF Gram's staining was positive in 62.5% patients and culture was positive in 40% cases. Bacterial agents isolated included pneumococci in 8(40%), staphylococci in 6 (30%), streptococci in 4(20%), H. influenzae in 4(20%), meningococci in 2(10%) and E. coli in 2(10%) patients. The pathogens isolated were highly susceptible to ceftriaxone in vitro (MIC 0.00006-0.008µg/ml) and the addition of 400 ng/ml dexamethasone to the broth medium had no effect. Forty established cases of bacterial meningitis were randomly assigned to either Group I (dexamethasone) or Group II (placebo) of 20 each. The overall clinical and laboratory characteristics of the two treatment groups were similar at the start of therapy (Table I). The administration of dexamethasone was associated with significantly rapid resolution of signs of meningeal irritation but no difference was found in two groups regarding resolution of fever, headache and vomiting. Occurrence of secondary fever, psychiatric manifestations and GIT bleeding were more frequent in dexamethasone group (p < 0.05) (Table II). Outcome : In Group I, out of 7 patients of papilledema, 2 recovered without complication, 3 recovered with complications and 2 expired. On the other hand out of 13 patients without papilledema, 12 recovered, only one developed complication and no mortality was observed (X2 = 9.134, p < 0.05); whereas in Group II, 9 patients with papilledema 3 expired, 5 had complications and only one recovered without complication. Out of 11 patients with normal fundus, one expired, 2 had complications and 8 recovered without any complication (X2 = 4.18, p = 0.2). Two patients died in Group I as compared to 4 in Group II (p< 0.05). All had pneumococcal meningitis. Neurological complications : At the time of discharge, 4 out of 18 patients (22.22%) in Group I had one or more neurological complication as compared to 6 out of 16 patients (37.5%) in Group II (p < 0.05). Complications included motor deficit, cranial nerve palsy, ataxia as well as CT scan abnormality like subdural empyema, cerebritis, cerebral infarction and hydrocephalus (Table III). Table III shows neurological sequelae recorded after discharge. Complications scores are shown in table II. The delayed hospital admission was one of the major factors that contributed to increased mortality and morbidity. Persistent severe sensorineural hearing loss was also significantly less common in dexamethasone group as compared to placebo group (p < 0.01) (Table IV). Discussion The development of meningeal inflammation in bacterial meningitis is not only due to the presence of live bacteria in subarachnoid space, but also due to the presence of bacterial cell wall components due to lysis of bacteria. These components induce the inflammatory response and increase blood brain barrier permeability, which leads to the exudation of serum protein in CSF. Tumor necrosis factor (TNF) is a macrophage secreted inflammatory mediator that is released in response to bacterial endotoxin, which further induces interleukin-1.15,16 Endothelial and macrophage released interleukin-1 acts as chemoattractant for neutrophils, causes the induction of proliferative response to glial cells and may contribute to brain gliosis scar formation and increased blood brain barrier permeability.17 However polymorphonuclear leukocytes accumulation in subarachnoid space by various mechanisms does not have any beneficial effect on host. On the other hand, it contributes to significant complications of bacterial meningitis. In this study the mean complications score was 6.33 ± 4.64 in dexamethasone group as compare to 9.8 ± 5.08 of placebo group (p <0.05). Similar results were obtained by Schaad et al,7 Girgis et al9 and Belsey et al.14 The overall neurological sequelae after recovery from meningitis were more in the placebo group than dexamethasone group. In the dexamethasone group, 14 out of 18 patients (77.77%) and in placebo group, 10 out of 16 patients (62.50%) recovered without neurological sequelae. In the present study, 4 patients in dexamethasone group had neurological sequelae, out of which one recovered at 45th day, another recovered at 90th day while 2 had persistent sequelae of moderate degree. On the other hand in the placebo group, 6 patients had neurological sequelae, one recovered at 45th days, one at 90th day and 4 had persistent sequelae of severe degree. This reflects the long-term beneficial effect of dexamethasone used as an adjunctive therapy for decreasing the long-term neurological sequelae and mortality. Dexamethasone decreases brain edema, intracranial pressure and increases cerebral perfusion to prevent regional hypoxia and focal ischemia of brain tissue5 along with reduction of inflammatory response in subarachnoid space in bacterial meningitis. Definite sensorineural (moderate to severe) hearing loss was seen in 4 patients out of 18 in the dexamethasone group (22.22%) as compared to 7 patients out of 15 in the placebo group (46.22%). Similar results were seen on follow up evaluation on 45th day. However, at 90th day, only 3 patients had moderate hearing loss in group I as compared to 5 in Group II. Two patients had profound hearing loss in the Group II and needed hearing aids (Table IV). These results are concordant with those of the studies by Schaad et al7 and Girgis et al.9 Pathogenesis of definite sensorineural hearing loss due to bacterial meningitis includes early purulent inflammatory involvement of cochlea and labyrinth.2 Several other mechanisms of hearing loss include (i) inflammatory spread from subarachnoid space to labyrinth leading to labyrinthitis (ii) nerve fiber damage due to ischemia (iii) direct damage to brain stem nuclei and upper hearing pathway.18,19 Meningeal inflammation in subarachnoid space is largely responsible for the pathophysiological consequences that are responsible for various clinical presentations and complications of acute bacterial meningitis through increased permeability of the blood brain barrier, cerebral edema (vasogenic, interstitial and cytogenic in origin), increased outflow resistance, cerebral vasculitis, increased intracranial pressure, decreased cerebral blood flow and loss of autoregulation of cerebral blood flow, cortical hypoxia that induce the inflammatory response.3 Thus it is concluded that adjunctive dexamethasone therapy improves some aspects of outcome of bacterial meningitis in adults by reducing the incidence of neurologic sequelae and sensorineural hearing loss. Mortality may also get reduced to some extent. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02015t3.jpg] [ni02015t2.jpg] [ni02015t1.jpg] [ni02015t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}