 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 68-70 Pneumatic Splints : Fabrication and Use in Neurorehabilitation A.B. Taly, K.P.S. Nair,* T. Murali,* M.Wankade* Departments of Neurology, Psychiatric
and Neurological Rehabilitation*, National Institute of Mental Health and Neurosciences,
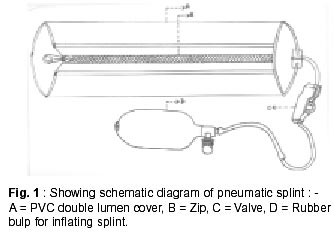
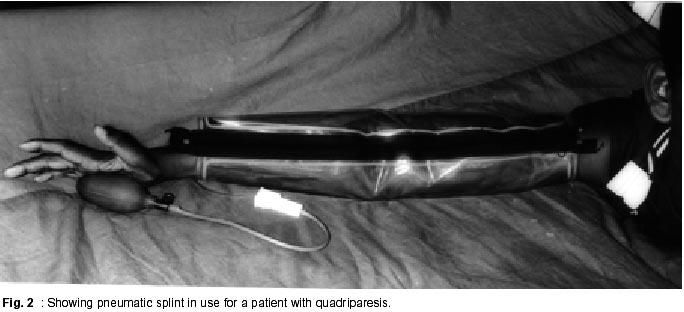
Bangalore - 560 029, India. Accepted for publication : 8th March, 2001. Code Number: ni02016 Summary Asymmetrical tone and weakness in antagonistic muscles often result in misalignment of joint, contractures and deformities. Traditional static splints used to prevent these complications are expensive, have to be custom made and cannot be used when deformities are marked. Authors describe fabrication and use of pneumatic splints, which are economic, safe and easy to apply. These splints have wide application in the management of common medical problems in neurological rehabilitation like hypotension, edema, pain, spasticity and early deformities. Key words : Deformities, Static splints, Pneumatic splints, Neurorehabilitation. Introduction Asymmetrical tone and weakness in antagonistic muscles due to neurological disorders often result in improper joint alignment. These can lead to contracture and permanent deformities, if not corrected. Splints are used to align the joints properly and prevent these secondary complications. However, there are several disadvantages of the commonly used conventional fixed splints. Besides being expensive, they have to be custom made, are difficult to fasten and cannot be used when deformities are marked. Tight splints can lead to pressure ulcers, particularly in patients with diminished or absent sensations. Further, these splints need to be redesigned with change in the neurological status of the individual. Air (pneumatic) splints make use of pneumatic pressure and are used in the treatment of variety of conditions like hypotension, edema, spasticity, pain and trauma. These splints are safe, easy to use and can be applied quickly. Currently, these splints are not manufactured in India and imported ones are expensive. Hence, an attempt was made to fabricate and test low cost air splints in patients with motor disability due to neurological disorders. Fabrication and application Pneumatic splints were made from polythene material. The measurements of the affected extremities were taken. Two pieces were cut from the large sheets, according to the shape and size of the affected limb. The sheets were welded together at the edges with a plastic welding machine. A one-way air valve was fixed to the outer sheet and a zip was attached to the free margin for fastening (Fig. 1). After proper positioning of the limb, the pneumatic splint was fastened. The splint was inflated with air pump from sphygmomanometer at pressures needed to align the joint correctly. Care was taken to maintain the inflation pressure below systolic blood pressure. The air was deflated and inflated at regular intervals to prevent ischemia and pressure ulcers. These splints were tried in preventing and correcting deformities at wrist, elbow (Fig. 2) knee and ankle joints. Any complications attributable to the pneumatic splints and problems in regular application were noted. These splints have been used in neurological rehabilitation facility for patients with stroke, head injury and spinal cord disorders. The cost of a splint was around Rs. 150 to Rs. 350 depending on the part affected and was less expensive than commercially available static splints. These splints were relatively 'dynamic' as compared to conventional fixed splints. These splints were easy to use and there were no complications like ischemia, pain, ulceration or compartment syndrome attributable to the splint in any of the patients. Client acceptability was good. Limitations such as problems in inflating and deflating the splint with air pump, air leaks and lack of durability were noted initially. Discussion Pneumatic pressure has been used in the treatment of various medical, neurological and orthopedic conditions. McKnight and Schomberg1 tried these splints in the treatment of rheumatoid arthritis and noted that air pressure resulted in reduction of pain, stiffness and swelling of hands and increase in the range of motion of the affected joints. In two prospective studies on edema after trauma, Thordarson et al2,3 noted that intermittent pneumatic compression was well tolerated and a useful adjunct for edema resolution. These splints may also be used to treat edema due to deep venous thrombosis and dysautonomia among patients with neurological disorders. Spasticity is a common problem among patients requiring rehabilitation e.g. stroke, head injury and myelopathies. Air splints were found to be useful in reducing the excitability of spinal motor neurons after stroke.4 Similarly, Robichaud and Agostinucci observed that circumferential pressure applied with air splint decreased alpha motor neuron excitability among patients with spinal cord injury.5 But this effect lasted only as long as the pressure was applied. Further studies are required to elucidate efficacy of pneumatic splints in the treatment of spasticity. Postural hypotension is common among patients with spinal cord disorders, peripheral neuropathies, Parkinson's disease and multisystem atrophy. Goudie et al studied the use of inflatable pneumatic splints for preventing hypotension during spinal anesthesia for cesarian section.6 Hypotension was less common and less severe among patients treated with pneumatic splints. These splints may also be useful for preventing postural hypotension. A study on the effect of pneumatic splints on postural hypotension among patients with neurological disorders is underway. It is necessary to maintain the pressure at optimal levels for splints to be effective, throughout the period of application. Solane and Dove studied the use of inflatable splints in ambulance services. They noted that these splints were not very efficient in holding the pressure and rapidly became ineffective. It is essential to have good quality valves to maintain the pressure with these splints.7 It was also noted that leak of air and subsequent loss of pressure is a common problem. Better valves and improved quality plastics could be used to overcome this problem. Ischemia is a potential complication of pneumatic splints. Christensen et al investigated the effect of pneumatic splint pressure on cutaneous oxygen tension. They noted that transcutaneously measured cutaneous oxygen tension decreased linearly with pressure in the splint and prolonged application of pneumatic splints at pressures above 15 mm Hg increased the risk of ischemia to limbs with fracture.8 Solane and Dove noted that therapeutic range between effective splinting pressure and ischemia is narrow.7 They recommended that 'blow-off valves' should be incorporated into such splints to avoid ischemia or compartment syndrome. Care should be taken to keep the splint pressure within therapeutic range. The limb should be inspected periodically for the evidence of ischemia. Regular deflation of the splints can prevent this complication. However, manual inflation and deflation of the splints at regular intervals requires manpower. Use of automatic pumps, which inflate and deflate the splints at pre-set intervals will help to overcome this problem. Such pumps are available but are expensive. Acknowledgement Authors acknowledge Mr. O.S. Chellapan, Instructor, plastic welding and molding section, for technical input in fabricating these pneumatic splints. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02016f2.jpg] [ni02016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}