 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 71-74 CASE REPORT Omental Transplantation for Temporal Lobe Epilepsy : Report of Two Cases H. Rafael, R. Mego, P. Moromizato,* W. Garcia* Department of Neurosurgery, Universidad Nacional Autonoma de Mexico
(UNAM), Departments of General Surgery and Anesthesiology*, Instituto Mexicano
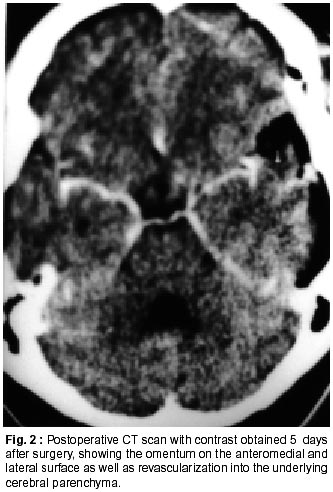
Del Seguro Social (IMSS)Mexico city, Mexico. Accepted for publication : 9th August, 2001. Code Number: ni02017 Summary The authors present two patients, with poorly controlled temporal lobe epilepsy, who received transplants of omental tissue on the anterior perforated space and left temporal lobe. At present, 26 months after the operation, the first patient has improved about 85 percent; whereas the second patient has complete control of seizures nine months after the operation. These clinical results indicate that epileptic seizures can be reduced or aborted with this new surgical modality (reconstructive technique). Key words : Complex partial seizures, Epileptogenic zone, Omental transplantation. Introduction The epilepsy surgery began in 1886, when Victor Horsley treated three patients with refractory seizures by surgical ablation of the epileptogenic zone.1 Since then and upto now, three essential procedures are used at many neurosurgical centers2-4 : i) surgical ablation, ii) disconnection procedures and iii) vagus nerve stimulation (palliative technique). However, since May 6, 1988 the authors have used a new surgical technique for patients with ischemic infarct and epilepsy.5,6 Two patients with poorly controlled epileptic seizures and treated by transplants of omental tissue on the epileptogenic zone are presented. Case Report Case 1 : A 33 year old right handed woman, had a 21 year history of medically refractory epilepsy. During these years, she had been treated with several antiepileptic drugs. Since 1995, she had received clonazepam 5 mg/day and oxcarbazepine 1200 to 1500 mg/day. During the last 3 years she had three spontaneous abortions between 6 to 13 weeks of pregnancy. During seizures she had tonic flexion of her right hand, palpitation, motor dysphasia and paleness, associated with partial impairment of consciousness for several seconds, and with a frequency of about 20 episodes per month. She also had 2-3 generalized tonic-clonic seizures per month, especially during the menstrual period. Postictally, she had moderate global dysphasia, memory impairment and headache for 30 to 60 minutes. In the interictal period, she had episodes of headache, irritability, motor dysphasia, sleep disorders and impairment of recent memory. Neurological examination revealed normal motor and sensory functions. Neuropsychological testing showed essentially recent memory impairment, slight motor dysphasia, irritability and agitation. Extracranial interictal electroencephalogram showed well localized epileptiform discharges in the left temporal region and, occasionally, generalized atypical spikes. A preoperative computerized tomography (CT) scan showed severe atrophy in both temporal lobes, especially in the left medial temporal lobe and probable heterotopia or sclerosis in a small area of the left temporo-occipital cortex. The clinical pre and postoperative picture was recorded on video tape, and the surgery was performed on April 18,1998 without complications. Case 2 : A 33 year old right handed man was admitted to hospital epileptic seizures, sleep disorders and progressive impairment of recent memory. During the last 28 years, he had been treated with many antiepileptic medicaments. Since 1997, he had received clonazepam 5 mg/day and sodium valproate 520 mg/day. He had olfactory hallucinations, palpitations, paleness, stuttering and partial impairment of consciousness for few seconds, with a frequency of about 12 episodes per month. He had 0-2 generalized tonic-clonic seizures per month. Postictally, he had moderate global dysphasia, memory impairment, headache and sickness for about two hours. In the interictal period, he had episodes of headache, stuttering, sleep disorders and lately, impairment of recent memory. Neuropsychological testing revealed frequent stuttering, agitation, anxiety and recent memory impairment. An interictal electroencephalogram revealed epileptiform discharges, most pronounced at the left temporal lobe. A preoperative CT scan showed moderate atrophy in both the temporal lobes, especially in the anteromedial portion of the left temporal lobe (Fig. 1). Surgery was carried out on September 7, 1999. Surgical Procedure : With the diagnosis of complex partial seizures with or without generalized tonicclonic seizures,7 due to a principal lesion in the medial temporal lobe, omental tissue (free omental flap with vascular microanastomosis) was transplanted on the anterior perforated space (APS) and left temporal lobe.8,9 An omental segment was placed on the APS (posterior and lateral zone) and medial surface of the left temporal lobe and another omental segment on the inferior and lateral surface of the same temporal lobe. Results In both patients, recent memory and sleep disorders improvement occurred on the third day after surgery. By June 2000, the first patient was having between 0-4 preictal seizures per month (earlier 20 months) and only five generalized tonic-clonic seizures during these 26 months postoperative (earlier 2-3 months). She is on clonazepam 3 mg in the night and oxcarbazepine 600 mg/day. During this postoperative course, the seizure occurred more frequently in the first few months; the severity and duration of epileptic attacks still being less than that before surgery. Moreover, in the intervening period, she had a pregnancy and normal delivery. Her postoperative CT scans (June 1,1999) showed the omental tissue on the medial and lateral surface of the left temporal lobe, as well as revascularization of the underlying cerebral parenchyma. The second patient, 9 months postoperative, had 80% improvement in stuttering. He was getting only clonazepam 2 mg at night. His postoperative CT scans (September 12, 1999) showed the omentum on the medial and lateral surface of the left temporal lobe as well as revascularization of the underlying brain (Fig. 2). During the nine months after the operation, this surgical technique led to a complete control of seizures. Discussion These results demonstrate that placing omental tissue directly upon the epileptic focus (medial temporal lobe structures) and neighbouring areas (posterior hypothalamus, subcommissural region and extreme superior of mesencephalic reticular nucleus), can reduce or abort complex partial seizures and confirm our previous clinical experiences5,6 as well as of other authors.10 The omentum11,12 is used because it is the best tissue to provoke the neoformation of blood vessels (revascularization) and through these vessels, the underlying and adjacent brain receives an increase in blood flow, oxygen, omental neurotransmitters (dopamine, noradrenaline and acetylcholine) and neurotrophic factors (nerve growth factor and gangliosides). Thus, the functional recovery of neurons and axons in the epileptic foci (residual nervous tissue)5,6 in ischemic and ischemic penumbra region can improve, if the blood flow is increased or reinstituted through the omentum. Therefore, interictal hypoperfusion13,14 and hypometabolism15 of the epileptic foci are normalized and likewise, extracellular concentration of glutamate and aspartate,16 and the neuronal hyperexcitability are reduced.13,17 Although pre and postoperatively regional cerebral blood flow was not measured by positron emission tomography (PET) or single photon emission computed tomography (SPECT) in the present two patients, the neurological improvement previously obtained after omental transplantation on the APS in patients with essential arterial hypertension,18,19 Alzheimer's disease,20 and late sequelae of the basal ganglia, the internal capsule and the thalamus8,9,12 demonstrate the efficacy of the transplanted omentum. In the author's opinion, the success of the pregnancy in the first patient was also due to a functional recovery of the neuronal hyper-excitability21-23 in the medial temporal lobe and its efferent projections via the fornix towards the neuroendocrine cells within the hypothalamus23,24 and subcommissural region.20,24 Conclusion The present two patients demonstrate that interictal focus must be revascularized in order to revert to the progressive hypoperfusion and hypometabolism, which produces increased epileptogenicity. Likewise, the authors believe that by means of this surgical procedure (reconstructive technique), the neuronal loss and the astrocytic gliosis can be stopped. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02017f2.jpg] [ni02017f1.jpg] |
| |||||||||

{kind=link}
{kind=link}