 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 81-83 CASE REPORT High Cervical and Lumbar Canal Stenosis of Varied Etiology : A Case Report M.J. Arunkumar, V. Rajshekhar Department
of Neurological Sciences, Christian Medical College and Hospital, Vellore - 632
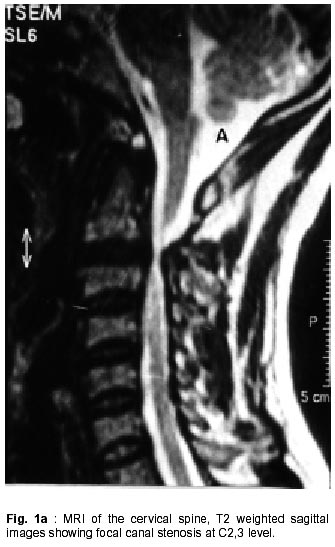
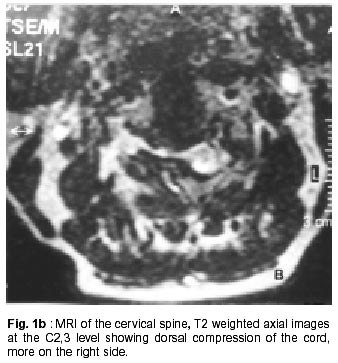
004, Tamil Nadu, India. Accepted for publication : 1st March, 2000. Code Number: ni02019 Summary Developmental stenosis without any significant spondylotic changes frequently occurs at C3 vertebra or below, and typically extends to C6-C7. However, high cervical focal canal stenosis is unusual. A case of cervical canal segmental stenosis at C2-3 level in addition to a developmental stenosis of the lumbar region, in a 45 year old male, has been presented in this article. The dynamics of the spinal canal in relation to the likely pathology of such conditions are reviewed. We speculate that focal segmental stenosis in the high cervical region may be due to a possible premature fusion of the neurocentral synchondrosis of the cartilage, or due to an abnormal rotary biomechanics which can result in facetal hypertrophy. Key words : Double stenosis, Cervical myelopathy, Neurogenic claudication, Pathology. Introduction Developmental canal stenosis with no radiological feature of spondylosis has been recognized by several authors as a cause of cervical myelopathy, which usually occurs below the level of the C3 vertebra. There are a few reports of high cervical canal stenosis, some at the level of the atlas,1 and the others at the level of the axis.2 Double canal stenosis involving both the cervical and lumbar spine is often developmental in origin.3 The authors present an unusual case of a high cervical myelopathy due to C2-3 focal stenosis caused by posterior arch elements with an associated lumbar canal stenosis. Case Report A 45 year old male presented with a history of paresthesias and numbness of the left lower limb with intermittent neurogenic claudication for a period of one year, right upper and lower limb weakness with stiffness associated with neck pain of six months duration and increased urinary frequency during the last two months. There was no history of trauma or metabolic disorders in the past. On examination, he had spastic weakness with grade 4/5 power in the right upper and lower limbs. In addition, he had weakness of the left extensor digitorum brevis and extensor hallucis longus. Light touch was impaired from C2 to T1 dermatomes on the right side; pain and temperature were impaired from the T8 dermatome to perianal region on the left side. Joint position sense and vibration sense were impaired over the lower limbs bilaterally. Deep tendon reflexes were exaggerated over the right upper and lower limbs with up going plantars; left upper limb reflexes were exaggerated while the left lower limb reflexes were diminished. There was mild tenderness over the lumbosacral and cervical spines. A diagnosis of a 'double stenosis' of the spinal canal was made, although the patient was more symptomatic due to the high cervical lesion. Magnetic resonance images (MRI) of the cervical spine showed focal canal stenosis at C2-3 level with myelomalacia (Fig. 1a and b). MRI of the lumbosacral region showed canal stenosis from L3 - L5. The patient underwent a C2-3 laminectomy and partial facetectomy on the right side. At surgery, the ligamentum flavum was found to be normal. The C3 lamina appeared buried underneath the C2 lamina which was hypertrophied. The right C2-3 facetal joints were hypertrophied, compressing the dural sac. As the patient was also symptomatic for lumbar canal stenosis, he underwent a L3 - L5 laminectomy, one week later. The facets were hypertrophied and medially placed causing indentation of the dural sac. He improved markedly in his symptoms, following the surgeries. Discussion Spinal canal stenosis as a significant developmental anomaly was described by Hinck et al in 1964.4 They suggested that the severity of neurological damage was influenced by the presence of developmental stenosis of the spinal canal.4 Spinal stenosis with significant reduction of the sagittal diameter of the spinal canal can exist in both the lumbar and cervical regions due to developmental changes associated with stress and aging. About 5% of these patients present with symptoms pertaining to both the lumbar and cervical regions and therefore require surgery at both or either of these levels.3 The initial diameter of the cervical spinal canal is the determining factor in the development of cervical myelopathy. Compression of the cord occurs if the initial diameter is 10 mm or less; it being uncommon with the diameter of more than 13 mm. At times, the normal spinal cord may have an antero posterior dimension of only 6 mm, and hence need not be compressed even in a 10 mm spinal canal. The narrower the canal, the greater will be the predisposition for cord compression secondary to trauma or acquired spondylosis. Flexion and extension of the neck can also alter the diameter of the cervical canal by about 2 mm.5 Abnormal rotary biomechanics may result in facetal hypertrophy which in turn can lead to canal stenosis.6 Premature fusion of the cartilaginous neurocentral synchondrosis can also lead to focal narrowing of the spinal canal by restricting the growth of the neural arch.2 Either or both of these factors can result in a high cervical focal stenosis. The present case had hypertrophied facets at C2-3 level, leading to focal stenosis in addition to a lumbar canal stenosis, probably of developmental origin. Abnormal rotary biomechanics leading to hypertrophy of the posterior arch element (the facets), together with a premature fusion of the neurocentral synchondrosis of the cartilage had probably led to a high cervical canal stenosis. It is worth mentioning that this patient was perfectly well till one year ago, and then became symptomatic. Therefore, the compressive myelopathy is likely to be due to either a trivial trauma to the neck (unnoticed by the patient himself) in the form of a hyperextension injury/subluxation, or the development of spondylotic changes in an already compromised cervical canal. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02019f1b.jpg] [ni02019f1a.jpg] |
| |||||||||

{kind=link}
{kind=link}