 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 84-86 CASE REPORT Germinoma of the Basal Ganglia : A Case Report and Review of Literature J. Elizabeth, G. Menon,* S. Nair,* R.N. Bhattacharya,* V.V. Radhakrishnan Departments of Pathology and Neurosurgery*,
Sree Chitra Thirunal Institute for Medical Sciences and Technology, Thiruvanthapuram
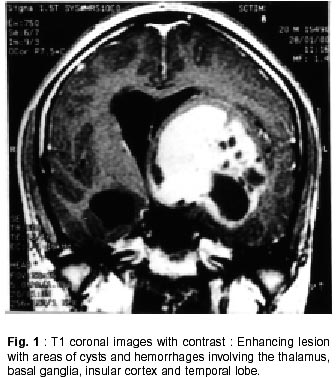
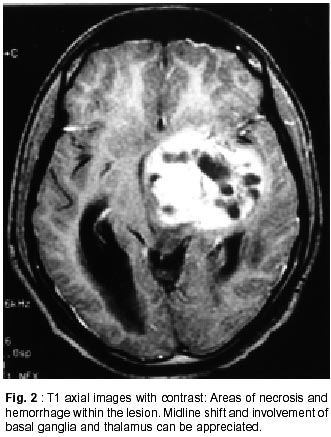
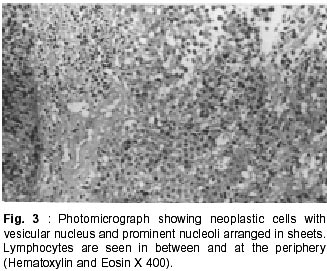
- 695 011, India. Accepted for publication : 9th October, 2000. Code Number: ni02020 Summary Germ cell tumors of extrapineal region are extremely uncommon. The clinicopathological features of germinoma in the left basal ganglia, in a 21 year old male are presented in this report. Post-operative radiotherapy is advocated, in view of the good radiosensitivity of these tumors. Key words : Germinoma, Germ cell tumor, Basal ganglia, Radiosensitivity. Introduction Intracranial germinomas constitute about 4.8% of all brain tumors in pediatric age group.1 The usual anatomical locations of these tumors are pineal, parapineal and suprasellar regions. The less common anatomical locations include intrasellar region, fourth ventricle, occipital region and cauda equina. Germ cell tumors originating in the basal ganglia are extremely uncommon and so far only 82 cases have been reported in the literature.1-7 In this communication, the clinicopathological features of germinoma arising from the left basal ganglia, in a 21 year old male patient are described. A literature survey indicated that this is the second case from Indian subcontinent.8 Case Report A 21 year old male patient presented with gradually progressive weakness of right side of the body for the past one year. This was accompanied by progressive difficulty in speech, headache and vomiting. There was no history of seizures or endocrine disturbances. Neurological examination revealed global dysphasia, bilateral papilledema, right sided lateral rectus palsy and right hemiparesis. Computed tomography (CT) scan showed a mixed density mass lesion in the left basal ganglia, extending into the thalamus, middle and inferior frontal gyrus and also into the superior and middle temporal gyrus (Fig. 1 and 2). Magnetic resonance imaging (MRI) revealed isointense lesion on T1WI and hyperintense lesion on T2WI. The lesion measured 6x6x5 cm in size and caused considerable mass effect and asymmetric hydrocephalus. The neuroradiological features were interpreted as a glioma arising from left basal ganglia - thalamic region. The patient was subjected to a left frontotemporal craniotomy. The tumor was predominantly in the basal ganglia and the thalamic regions, and was extending into the insular cortex and the temporal lobe. An anterior temporal polectomy was done, as the tumor was seen extending into the temporal lobe. Thereafter, tumor decompression was done through a transsylvian approach. An adequate decompression could be achieved through this approach, as the tumor started falling into the decompressed cavity. The tumor was fleshy, moderately vascular and suckable with areas of cystic change containing hemorrhagic fluid. In the immediate postoperative period, the patient showed minimal improvement in his aphasia and hemiparesis. He was discharged on the eighth postoperative day and was referred to radiotherapy department. He received a combination of radiotherapy and chemotherapy for a period of one year. MRI scan, after a year of surgery showed no demonstrable lesion. Neurologically, he still had aphasia and hemiparesis. Histologically, the tumor was composed of sheets of cells. The individual neoplastic cells were polyhedral with abundant clear or eosinophilic granular cytoplasm and round large nucleus with prominent nucleoli (Fig 3). Occasional mitotic figures were also seen. Imperceptibly merging with these cells were small groups of lymphocytes displayed in and around vascular channels and along fibrous septa. No other germ cell components like choriocarcinoma, yolksac tumor, teratoma etc were present and because of that immunohistochemical markers for AFP, CEA, and HCG were not considered essential. These histological features in the surgical specimen were interpreted as germinoma arising from the basal ganglia. Discussion Germinomas originating in the non-midline structures within the central nervous system are uncommon. The reported incidence of germinoma of the basal ganglia varies between 5-10% among all intracranial germinomas.1 Of the non-midline germ cell tumors, those arising with in the basal ganglia are most often germinomas, whereas those arising from fourth ventricles are reported to be non-germinomatus germ cell tumors.9 Patients with germinoma of basal ganglia usually manifest with gradually progressive hemiparesis. Signs of raised intracranial pressure are usually not present, because these tumors are not invasive and do not obstruct the ventricular system. However, our patient had features of raised intracranial pressure as well as showed asymmetric hydrocephalus on the MRI scan. Some of the patients with germinoma of basal ganglia, particularly of longer duration, may present with features of cerebral hemiatrophy. The cerebral hemiatrophy is regarded to be due to the Wallerian degeneration of afferent fibres from the thalamus.10,11 Liu et al2 recently reported markedly elevated antiphospholipid antibodies in a patient with germinoma arising from basal ganglia and they suggested an autoimmune pathogenesis for the progressive cerebral atrophy. Higano et al7 reported an incidence of cerebral atrophy in 50% of their cases. The tumor in the basal ganglia may at times extend to the hypothalamus and in such instances patient may present with features of poikilothermia.12 Although a spectrum of neuroimaging features have been described in the earlier reports, there are no specific features on MRI, by which germinoma of basal ganglia can be diagnosed with any degree of certainty. Intracranial germinomas in contrast to other germ cell tumors like teratoma, respond very well to radiotherapy and chemotherapy. It is, therefore, essential that accurate histopathological diagnosis of germinoma should be made for an early treatment as well as minimising the sequelae. At times, in a small or fragment biopsy material, the lymphocytic component may be minimal or even absent. Tissue artifacts during the surgery due to thermocoagulation as well as during histopathological processing may distort the characteristic morphological appearances of these tumors. Germinomas are usually negative for AFP, CEA or HCG. It is being reported that some germinomas containing syncytiotrophoblastic giant cells may be positive for HCG, but this has no prognostic significance.13 The occurrence of non-midline intracranial germinomas may be the result of midline streaming of totipotent cells, early in the neural tube development. The development of third ventricle may result in the deviation of ectopic germ cells from the midline and these ectopic germ cells manifest their occurrence in the basal ganglia. There is usually no genetic background for the occurrence of germinomas in basal ganglia. However, isolated cases of germinoma of basal ganglia have been reported in association with Down's syndrome.3,14 The occurrence of germinoma of basal ganglia in siblings has been reported by Aoyama et al.15 References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02020f1.jpg] [ni02020f3.jpg] [ni02020f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}