 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 1, March, 2002, pp. 87-89 CASE REPORT Familial Trigeminal Neuralgia V. Gupta, A.K. Singh, S. Kumar, S. Sinha Department of Neurosurgery, G.B. Pant
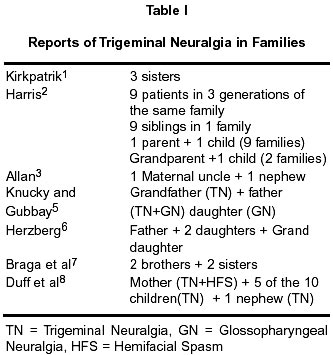
Hospital, New Delhi, India. Accepted for publication : 31st March, 2000. Code Number: ni02021 Summary Familial trigeminal neuralgia is infrequent. A report of a couple and their son being afflicted by this malady is presented. The clinical features, radiological findings and surgical management are discussed and literature reviewed. Key words : Trigeminal neuralgia, Microvascular decompression. Introduction Trigeminal neuralgia is characterized by the presence of unilateral, excruciating pain in the distribution of one or more branches of trigeminal nerve. Classically, it is known to occur in a sporadic fashion without epidemiological or genetic significance.1 A family history of trigeminal neuralgia is uncommon. There are isolated case reports of familial clustering of trigeminal neuralgia in the literature,1-8 that suggest occurrence in blood relations, in offsprings or siblings. The authors report an unusual clustering occurring in a non-consanguineously married couple and their son. All of them were operated upon for microvascular decompression of trigeminal nerve at G. B. Pant Hospital, New Delhi, in the last two years. Case Report Case 1 : A 62 year old lady was admitted in Neurosurgery department with history of severe, burning, lancinating pain in right V1 and V2 divisions of the trigeminal nerve for the last twenty years. Pain was provoked by mastication and speech. She initially had relief with carbarmazepine but later become refractory to drugs. Her neurological examination was normal except for slight hyperesthesia in right malar region in the V2 division. A CT scan of the skull was unremarkable. She underwent microvascular decompression of trigeminal nerve by retromastoid craniectomy. Anterior inferior cerebellar artery (AICA) was found to be compressing the nerve at root entry zone (REZ). The offending vessel was moved away using a dural substitute (Preclude) loop and anchored to the tentoruim, using dural clip. Her postoperative course was uneventful and she became pain free and continues to be so, without medication. Case 2 :A 38 year male, elder son of case 1, presented with history suggestive of classical trigeminal neuralgia in right V1 and V2 divisions of trigeminal nerve, for the last 2 ½ years. Pain came on with exposure to cold wind, speech, and mastication. On examination, no neurological deficit could be elicited. CT scan of the head was normal. He was operated upon by right retromastoid craniotomy and microvascular decompression (MVD) was done. Superior cerebellar artery (SCA) was found to be compressing the REZ of trigeminal nerve; the vessel was dissected free and moved away. A piece of dural substitute (Preclude dura) was interposed between them to maintain decompression. He was relieved of pain after surgery but was afflicted with vertigo, which subsided over next two weeks. He was pain free without medication at follow up after thirteen months. Case 3 : A 65 years old man, husband of case 1 and father of case 2, had also been suffering from trigeminal neuralgia in right V1and V2 distribution for the last one year. On examination, there was hypoesthesia in right V2 division. CT scan head was normal. MRI brain for posterior fossa neurovascular relationships did not reveal any compression. At surgery, the offending vessel was superior petrosal vein. Microvascular decompression was done and a dural substitute (Preclude dura) graft was used to maintain separation. Post operatively, patient's pain got reduced in intensity but he had to be given carbamazepine which completely relieved him. Discussion Reports of trigeminal neuralgia occurring in more than one member of the same family are rare. Few reports of trigeminal neuralgia occurring in families1- 8 (Table I) and two reports of secondary trigeminal neuralgia occurring in families associated with Charcot-Marie-Tooth disease could be found in literature.9,10 We did not find any report of familial trigeminal neuralgia occurring in a couple who, though a family, are not blood relatives. This unique occurrence may suggest some unknown common factor e.g. environmental, dietary or just plain coincidence. The affliction of their son by the same disease, (while the two younger offsprings were spared) is still interesting. Current knowledge about pathophysiology and etiology of trigeminal neuralgia is limited. There is a lively debate going on between those who believe in a peripheral cause, i.e. vascular cross compression of a root exit/entry zone causing ephaptic transmission, 11,12 and those who believe that all hyper dysfunctional syndromes are caused by a central cause, as they often respond to anticonvulsants.13,14 Moreover, vascular compression has also been found in asymptomatic individuals at autopsy.15 There appears to be a small but significant group of patients, where no convincing evidence of vascular compression has been found at surgery. Moller,16 in a recent review, speculated that in addition to vascular compression there may be a second unknown factor, which may cause trigeminal neuralgia. Kirkpatrik1 observed that if the disease is truly random, then such familial clustering would be infinitesimally rare, but this does not seem to be the case. He postulated that there appears a specific organic or anatomic cause of trigeminal neuralgia that usually occurs sporadically, but is occasionally consistent in certain genetic groups. Familial clustering of trigeminal neuralgia has been noted to be more common in women1,6,17,18 thus leading to the speculation of dominant pattern of genetic transfer. Familial trigeminal neuralgia has been reported in association with Charcot Marie Tooth disease9,10 and with multiple sclerosis (MS).2 All the three individuals in the present report had no neurological symptoms suggestive of any demyelinating disease nor were they investigated for the same. All three had computed tomography of skull and one (case 3) had MRI brain, which, however, showed no evidence of MS. Harris2 noticed familial trigeminal neuralgia in 40 out of a total of 1,433 cases (2%), in which heredity possibly played some role. In 6 of these 40 cases (20%), the neuralgia was bilateral. In one family, he found nine sufferers in three generations and nine patients as siblings in one family or grand parent along with an offspring was afflicted in two families. He observed that cases in subsequent generations occurred at earlier age. This seems to be the case in the present family as well. The mother was affected at the age of 42 years and the father at 74 years, whereas their son got affected at 32 years of age. Kirkpatrik1 suggested that the mechanism of trigeminal neuralgia in these familial patients is somewhat different from that of a typical patient, or it may be that the mechanism is the same, but some unknown factor influences final common pathway. He postulated premature atherosclerosis of vascular network of posterior fossa, with ectasia causing kinking of the vessel leading to vascular compression of the nerve. The occurrence of familial vascular malformations or aneurysms has also been recognized. Other pathological conditions suspected to be associated with familial trigeminal neuralgia include genetically inherited abnormal myelin which is more susceptible to pulsatile compression, prior illness such as systemic vasculitis, or viral disease. Skull base structures causing crowding in posterior fossa and hence increasing the possibility of neurovascular compression has also been postulated. However, no bony abnormality was seen in any of our patients. In none of the cases reported earlier, the affected patients were subjected to surgery as not all members of reported families were living in the same city, and were afflicted over long periods of time. They were treated by different physicians by different modalities, whereas in all the three case reported here, a vascular compression was found and microvascular decompression was done. Therefore, to conclude, we think that the etiology of trigeminal neuralgia can be multifactorial and different factors may operate in different groups of patients. This report only intends to highlight a genetic cause as well as a possibility of a second, unknown cause, like an environmental or a dietary factor, in the said family. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02021t1.jpg] |
| |||||||||

{kind=link}