 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
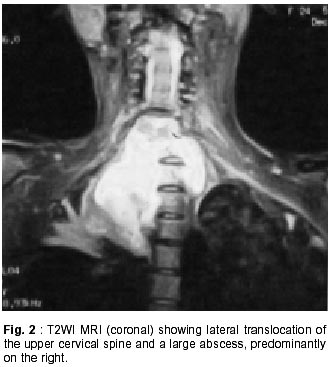
Neurology India, Vol. 50, No. 1, March, 2002, pp. 93-94 SHORT REPORT Cervico Thoracic Junction Spinal Tuberculosis Presenting as Radiculopathy D. Gopalakrishnan, K.N. Krishna Correspondence to : Dr. D. Gopalkrishnan, 81/1 East, Anjaneya Temple Road, Basavanagudi, Bangalore - 560 004, India. Code Number: ni02023 Summary A case of cervico thoracic junctional area spinal tuberculosis presenting as painful radiculitis of the upper extremity is reported. The predominant symptom of radicular pain and muscle weakness in the hand, along with a claw deformity, led to considerable delay in diagnosis. The presence of advanced bone destruction with severe instability was demonstrated on the MRI scan done later. Surgical management by radical anterior debridement and fusion, along with chemotherapy, led to resolution of the upper extremity symptoms. The brachial plexus radiculopathy secondary to tuberculosis has not been reported. The absence of myelopathic signs even in the presence of advanced bone destruction, thecal compression and instability is uncommon in adults. Key words : Spinal tuberculosis, Cervico thoracic junction, Radiculopathy. Introduction Tuberculosis affecting the junctional areas of the spine eludes early diagnosis. The anatomical location precludes proper visualization by conventional radiography unless special care is taken. The problem is compounded when local symptoms are overshadowed by peripheral symptoms due to pathological process, leading to a considerable delay in diagnosis. Cervico thoracic junction tuberculosis constitutes 5% of spinal tuberculosis1 and usually presents with local symptoms of pain and bony deformity with or without features of neural compression. A case of cervico thoracic junction tuberculosis presenting with the predominant symptom of a unilateral painful radiculopathy of the upper extremity with motor weakness and clawing of the hand, which overshadowed the local pain in the neck, is reported. Features of spinal cord compression were absent inspite of delay in diagnosis and advanced bone destruction. Case Report A 24 year old girl presented with intractable pain in the left upper limb, weakness of the hand and pain in the root of the neck. Symptoms had started eleven months back with predominant radicular pain in the median and ulnar nerve distribution. She had been investigated for this and found to have a raised ESR (90 mm/hr), a normal cervical spinal radiograph, and ENMG findings of axonopathy in the left median and ulnar nerves. Treatment with oral steroids and carbamazepine did not provide any relief. Eight months later, she developed fever and cough. On admission to our spine services eleven months after the onset, she was found to be in severe pain, and was unable to lie supine or on her left side. She was emaciated and toxic. Clinical examination revealed a median and ulnar claw deformity of the left hand with wasting of all muscles of the hand. A tender gibbus was found at the cervicothoracic junction. The motor power was 2/5 in the C8-T1 innervated muscles of the left hand along with sensory hypoesthesia in the left C6-C8-T1 dermatomes. There were no pyramidal signs. Plain radiograph of the cervical spine revealed destruction of the vertebrae at the cervico thoracic junction. MRI of the cervicothoracic junction revealed destruction of the seventh cervical and first and second thoracic vertebrae, with a prevertebral and anterior epidural soft tissue mass suggesting tuberculous destruction with abscess formation. The abscess was predominantly on the right side, extending over the lung apex. There was translocation of the upper cervical spine laterally to the right and anteriorly (Fig. 1 and 2). After improving her general condition, surgical exploration of the spinal lesion by an anterior low right Southwick and Robinson approach was done. Excision of the medial end of the clavicle or splitting of the manubrium was not needed, as on entering the abscess cavity it was easy to access the destroyed vertebrae. Drainage of the abscess and radical debridement by corpectomy of C7, T1 and T2 was followed by anterior fusion from C6 to T3 with tricortical iliac crest graft. Histopathology confirmed the tuberculous nature of the lesion and treatment with four drug antituberculous chemotherapy was started. There was significant relief of pain in the upper limb in the immediate postoperative period. She was mobilized on a Somi brace after three weeks. At one year follow-up, bony fusion had been achieved, there was no radicular pain in the upper limb and the motor power in the left hand was 4/5. Discussion The predominant symptom of radiculitis of the lower trunks of the brachial plexus, with presentation like brachial neuritis, which overshadowed the local spinal pain, lead to a delay in diagnosis. There were no clinical signs of spinal cord compression inspite of the magnitude of destruction, dislocation and abscess formation. Hsu and Leong1 noted that cervical tuberculosis presented in two ways. In children below ten years, there was diffuse and extensive involvement with formation of large abscesses but a low incidence of paraplegia. The adult type was more localized with a paucity of pus and a higher incidence of paraplegia. Our patient, though being 24 years old, would seem to have the former type of involvement, which is unusual. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02023f1.jpg] [ni02023f2.jpg] |
| |||||||||

{kind=link}
{kind=link}