 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
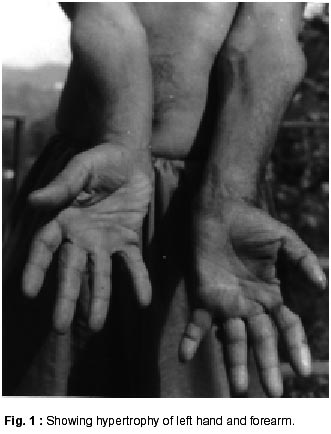
Neurology India, Vol. 50, No. 1, March, 2002, pp. 95 SHORT REPORT Syringomyelia as a Cause of Limb Hypertrophy J. Mehta, S. Khanna Correspondence to : Dr. J. Mehta, Department of Neurology, Indira Gandhi Medical College, Shimla-1, H.P., India. Code Number: ni02024 Summary A case of limb hypertrophy secondary to syringomyelia is presented. Key words: Syringomyelia, Limb hypertrophy. Introduction Syringomyelia is classically associated with segmental weakness and wasting (generally involving the hand and arm) with loss of tendon reflexes and segmental dissociated anesthesia. We are presenting a case of syringomyelia with limb hypertrophy, instead of atrophy. Case Report A 54 year old, right handed male was seen in the neurology department with the complaints of decreased sensations on the left half of the face, arm and chest for the last 36 years. He had gradually progressive history of objects falling from left hand without knowledge and proximal as well as distal weakness of left upper limb. He had insidious onset unsteadiness of gait of 7 years duration. There was no history of cranial nerve involvement or sensory symptoms in the lower limb. There was no history of spinal injury or meningitis. General examination revealed a short statured patient with thoracic kyphoscoliosis and convexity to right. There was a localized painless swelling in the region of left arm suggestive of rupture of tendon of biceps brachii. The left elbow showed a painless swelling with crepitus and restriction of movements i.e. Charcot's joints. There were scars and burns on the fingers. Neurological examination showed normal higher mental functions, left Horner's syndrome, decreased sensation on left half of face, loss of taste sensation on left half of tongue, left 9th and 10th cranial nerve palsy. Left sternocleidomastoid and trapezius were weak. The tongue showed wasting, fasciculations on left half and deviation to left on protrusion. Motor system examination revealed hypertrophy of left hand and forearm (Fig. 1). There was difference of 3 cm in the forearm girth. Fasciculatory tremors were seen on the left hand fingers. There was hypotonia of left upper limb and normal tone in other extremities. Power was grade 3 to 4 in left upper limb, 4 to 4+ in left lower limb, 4+ in right lower limb and 5 in right upper limb. Deep tendon reflexes revealed absent left biceps, triceps and supinator reflexes. The plantars were extensor bilaterally. Sensory examination revealed loss of hot cold sensations and pain on left arm and left half of chest. Position sense was lost in left upper limb. MRI of the brain and spine (T1, T2, Proton PD sequences) revealed grade 1 Arnold Chiari malformation with long syrinx extending from cervico-medullary junction to T6 (Fig. 2). X-ray of the hand did not reveal any bony hypertrophy. A syringosubarachnoid shunt was done. There was no fresh deterioration in neurological status, after the surgery. Discussion The association of hypertrophic changes in bones, muscles, other tissues especially upper limb has been recognized in syringomyelia.1,2 Kazumasa et al2 described limb hypertrophy in 11.5% of cases in their series. In our experience of 25 cases, this is the first case. Different mechanisms have been postulated for neurogenic hypertrophy in syringomyelia. These include stimulation of sympathetic nervous system3 causing defective circulation and edema. Delaporte et al4 postulated that muscle hypertrophy occurring in syringomyelia is secondary to neural abnormalities. These result in release of molecules which accelerate proliferation and protein synthesis rates in muscle cells involved in the development of hypertrophy. In this case, it seems that combination of factors i.e. stimulation of pre-ganglionic sympathetic neurons in the intermediolateral columns, as well as anterior horn cells stimulation by the syrinx cavity, may have been responsible. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02024f2.jpg] [ni02024f1.jpg] |
| |||||||||

{kind=link}
{kind=link}