 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
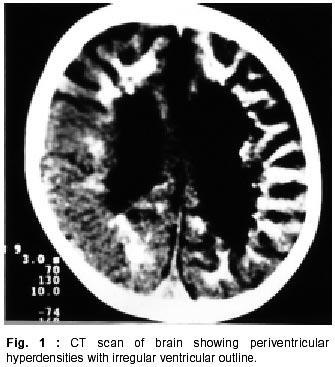
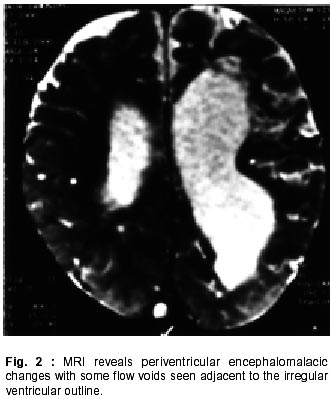
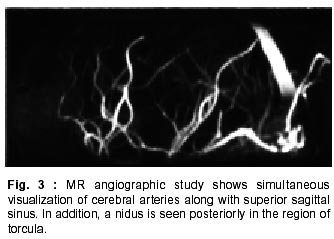
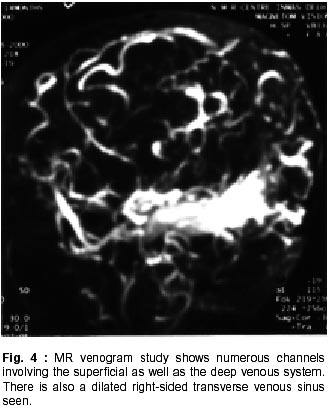
Neurology India, Vol. 50, No. 1, March, 2002, pp. 96-97 SHORT REPORT Atypical Manifestation of Dural Arteriovenous Fistula R.P. Tripathi, S. Gupta, M. Taneja, S. Kaushik, Prabhjot Kaur Correspondence to : Dr. M. Taneja, NMR Research Centre, Institute of Nuclear Medicine and Allied Sciences, Lucknow Road, Delhi - 110 054, India Code Number: ni02025 Summary A case of secondary dural arteriovenous fistula presenting as infantile stroke, in a fifteen month old boy, is reported. The initial impression on CT scan in this case was misleading, due to the atypical appearance of the pathological periventricular blood vessels, interpreted as periventricular calcification. Key words : Dural arteriovenous fistula, Hypoxic ischemic encephalopathy, MR angiography. Introduction Dural arteriovenous malformations of the transverse sinus are relatively localized to the occipitomastoid regions and occur predominantly in women who are more than 40 years of age.1 Most of the dural malformations are acquired abnormalities, unlike parenchymal malformations, which are congenital lesions. These malformations have been known to arise as complication of sinus thrombosis.2-4 Dural arteriovenous fistulas (DAVF) associated with venoocclusive disease and dilated pial venous drainage can be documented on MRI. Case Report A 15 month old boy presented with a history of inability to sit. He kept rolling over when ever on bed. The child was born prematurely, had delayed developmental milestones and had right sided hemiplegia. CT scan revealed dilated lateral and third ventricles with a compressed fourth ventricle. The lateral ventricular walls revealed irregularities along with prominent periventricular hyperdensities, which were interpreted as periventicular calcifications (Fig. 1). MRI revealed a dilated lateral ventricle with irregular outline and a dilated third ventricle with a normal aqueduct and compressed fourth ventricle. There were periventricular encephalomalacic changes and no evidence of calcification on any of the imaging sequences (Fig. 2). There was an irregular hyperintense signal on T1WI in the region of torcula herophili. The right-sided transverse sinus was prominent. The region of torcula and fourth ventricle also revealed few irregular areas of flow voids. MR angiography revealed simultaneous filling of the major cerebral arteries and its branches along with the superior sagittal sinus (SSS) (Fig. 3). In addition, the posterior end of SSS showed an area of signal loss extending into the region of torcula and a dilated right transverse sinus, which was due to a thrombus. There were multiple collaterals seen in the adjacent area including vessels from ECA branches. The above findings suggest an episode of thrombosis in the torcula and right sided transverse sinus with the secondary formation of a DAVF. MR venogram revealed a loss of the normal venous anatomy with grossly dilated and tortuous numerous channels involving the superficial and deep venous system, (Fig. 4), which simulated calcification on CT scan. The posterior aspect of SSS was not discernible with numerous collaterals adjacent to it. DSA study done subsequently confirmed the findings. Discussion DAVFs can be classified into two major groups: cavernous sinus DAVFs (CS-DAVFs) and noncavernous sinus DAVFs (NCS-DAVFs). Approximately 30% of symptomatic intracranial DAVFs involve the transverse and sigmoid sinuses.5 DAVFs are uncommon in children. They usually present at an older age, with clinical features depending on their location in the brain. In this case, the presentation was with childhood hemiplegia with delayed developmental milestones in a premature child. The clinical impression was of a sequelae of hypoxic-ischemic encephalopathy or possibly a TORCH infection. The ventricular dilatation in this case was due to an ectatic vessel compressing the fourth ventricle. The main clue to the diagnosis of the etiology in this case was the area of hyperintensity in the region of torcula on MRI with asymmetry and signal loss of the cerebellum on the right side which was later confirmed on MR angiogram, to be due to the thrombosis affecting the region of torcula and extending into the right transverse sinus.6 The arterial supply to the DAVFs of the transverse and sigmoid sinuses is via branches of the external carotid artery.7 The nidus is located in the sinus wall with immediate shunting of blood. The symptoms and the imaging findings of encephalomalacic changes are explained on the basis of venous shunting of blood with backpressure changes. The etiology of the fistulous communication appears to be sinus thrombosis.4 DAVFs are uncommon in young children with atypical clinical presentation. In this case, we found a secondary DAVF in a young child, following a thrombus in the region of torcula and the adjacent right-sided transverse sinus. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02025f4.jpg] [ni02025f2.jpg] [ni02025f3.jpg] [ni02025f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}