 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
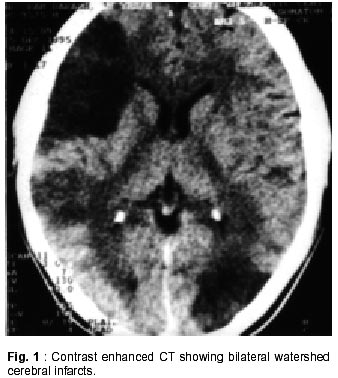
Neurology India, Vol. 50, No. 1, March, 2002, pp. 100-101 SHORT REPORT Scorpion Bite and Multiple Cerebral Infarcts A.K. Thacker, R. Lal, M. Misra Correspondence to : Dr. A. Thacker, Department of Neurology, B.R.D. Medical Sciences, Gorakhpur, - 273 013, India. Code Number: ni02027 Summary Multiple cerebral infarcts, bilateral optic neuropathy with limb ischemia, following scorpion bite is documented. Vasospasm and autonomic storm due to envenomation is a plausible explanation for this symptom complex. Key Words : Scorpion bite, Cerebral infarcts. Introduction The systemic manifestations of scorpion bite are a result of intracellular influx of Na+ and Ca++ ions through sodium channels with resultant autonomic storm.1,2 The clinical manifestations of this venom thus include hypertension, pulmonary edema, myocardial hypoperfusion and death. Scorpion venom is water soluble antigenic mucopolysaccharide with low molecular weight molecule releasing histamine and neurotoxins.3 Cerebrovascular complications, following scorpion bite are rare. While coagulins present in the venom or DIC may induce intravascular thrombosis,4 intracerebral hemorrhage may follow an acute rise in blood pressure.5,6 This case report illustrates multiple cerebral infarcts, limb ischemia and bilateral optic neuropathy on scorpion envenomation. Case Report A 17 year old male farmer was bitten by a scorpion in the field. The description favoured red scorpion, (Buthus tumulus), the species most prevalent in the region. He was given local xylocain injection, which controlled the pain. In the night he developed severe breathlessness which was relieved with diuretics. Next morning he noticed diminished vision in the left eye. The patient was referred to us on the third day of envenomation with the findings of listless and weakness of left upper and lower limbs. On examination, he was stuporous, responding only to painful stimuli. His right radial, brachial, subclavian and carotid pulses were not palpable, while those on the left were normal. Blood pressure too could not be recorded over the right arm but was 120/70 mmHg on the left. The lower limb pulses and the blood pressures were normal and equal on both sides. His right upper limb was cooler compared to the left, although there was no pallor, cyanosis or gangrene. The examination of respiratory, cardiac and abdomen were normal. Neurologic examination revealed a stuporous patient with right gaze deviation. The left pupil was slightly large compared to the right and reacted sluggishly to light. Fundus examination was normal on the right but showed disc and retinal edema with perimacular hemorrhage on the left. He had left hemiparesis (power 2/5 in the upper and 0/5 in the lower limb). Blood counts, hemogram, bleeding time, cephelin clotting time and fibrin degradation products level were normal. Blood biochemistry (for sugar, creatinine, bilirubin, liver enzymes and electrolytes) ECG, chest x-ray and CSF cytology and biochemistry were also within normal limits. Contrast enhanced CT scan showed multiple bilateral triangular watershed cerebral infarcts involving the frontoparietal regions anteriorly and temporo-occipital regions posteriorly in the distribution of the middle cerebral artery especially on the right (Fig. 1). 2D color doppler study of the heart, normal. The cardiac chambers and valves, with no clot or intracavitory mass. The aortic arch, the origin and proximal segment of the brachiocephalic, left carotid and subclavian arteries were structurally normal with aortic flow velocity of 70 cm/sec, distal to the left subclavian artery. The patient was treated with IV fluids and dexamethasone 4mg IV 8 hourly. His conscious improved slowly over next 2 weeks but he noticed deterioration of vision in both eyes. Fundus examination showed bilateral disc pallor with perimacular hemorrhage and pigmentary retinal degeneration on the left. By the tenth week, he was able to walk with residual left hemiparesis. The arteiral pulsations in the right arm and the carotids were palpable normally but blindness of the left eye persisted. Discussion Multiple bilateral asymmetric watershed cerebral infarcts as seen in the present case are likely to be due to reduced blood flow in the carotid arterial system. Low flow infarcts from carotid occlusions are predominantly unilateral with subcortical anterior boundary lesions leading to contralateral weakness which is worse in the leg.7 The reduced carotid blood flow in the present case can perhaps be explained by severe vasospasm related to autonomic storm following the scorpion bite. Catecholamine excess, with firing of alpha receptors, enhances endothelin secretion with severe vasoconstriction.8 Additionally, the right upper limb ischemia and the retinopathy can be related to the vasospasm secondary to autonomic hyperstimulation of retinal vessels and the right upper limb blood vessels. Myocarditis and thrombo-embolic phenomena following scorpion bite are also known to give rise to cerebral ischemia. These explanations are less likely in this patient with normal hematologic parameters, normal doppler studies of the vesels and with no electro or echocardiographic evidence of myocarditis or intracardiac thrombosis. Spontaneous recovery of the cerebral and limb ischemia in the patient favour vasospasm as the main cause. Drugs with sympathomimetic activities such as amphetamine and cocaine have been associated with similar cerebral infarcts and optic neuropathy.9 The pathogenesis of such cerebral infarctions has been related to the potent vasoconstrictive properties of these drugs. Scorpion envenomation too induces hyper catecholinemia and autonomic storm following activation of sodium channels and excessive neuronal activity.10 Scorpion bites may be associated with initial short lasting hypotension secondary to bradycardia and hypovolemia caused by perspiration and vomiting due to acetyl choline excess.11 The acute dyspnea on the night of scorpion bite could have been due to pulmonary edema, a known complication of envenomation. The associated hypotension possibly precipitated the cerebral ischemia in the already compromised carotid circulation due to vasospasm. The cerebral infarcts, clinically evident 36 hours after the envenomation, are compatible with low flow infarcts, which are known to develop and progress gradually over days or week.12 References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02027f1.jpg] |
| |||||||||

{kind=link}