 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
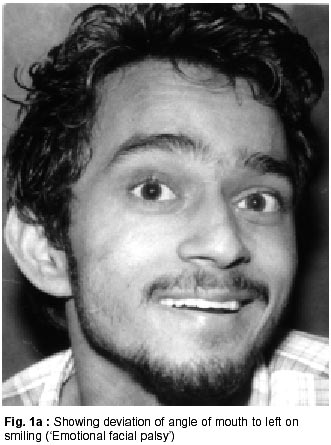
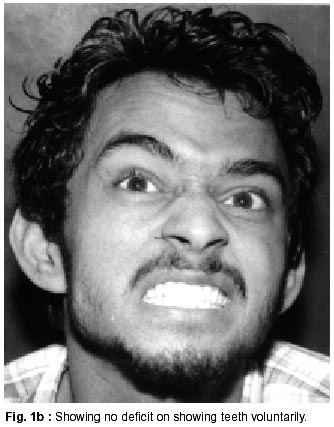
Neurology India, Vol. 50, No. 1, March, 2002, pp. 102-104 SHORT REPORT A Case of Emotional Facial Palsy with Ipsilateral Anterior Inferior Cerebellar Artery Territory Infarction D. Khurana, V.R. Sreekanth, S. Prabhakar Corespondence to : Dr. D. Khurana, Department of Neurology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India. E-mail : dherajk@yahoo.com Code Number: ni02028 Summary Emotional facial palsy (EFP) commonly results from anterolateral thalamic or striatocapsular infarcts. Its occurence in brainstem lesions is uncommon, with previously reported cases being restricted to superior cerebellar artery infarction (3 cases). We report an unusual case of EFP ipsilateral to an anterior inferior cerebellar artery infarction, which opens new insights into the facial corticobulbar tract pathway. Key words : Emotional facial palsy, Anterior inferior cerebellar artery infarction, Brainstem stroke. Introduction Emotional facial palsy (EFP) refers to weakness of facial movements during emotions like smiling or weeping, while voluntary movements do not show any deficit. EFP has been described in association with lesions in the contralateral supplementary motor area,1 striatocapsular region, thalamlus and subthalamus, Parkinson's plus syndrome and postencephalitic parkinsonism.2-5 EFP associated with pontine infarction is rare in occurrence. Three patients with EFP in association with superior cerebellar artery (SCA) infarction have been previously reported.6 We report a case of EFP in association with anterior inferior cerbellar artery infarction - an entity not previously described. Case Report A 20 year old male presented with recurrent episodes of vomiting, dizziness, along with nasal regurgitation of fluids and slurring of speech. Examination revealed ocular dipping, right sided emotional facial palsy (Fig. 1a and b), right palatal weakness, an extensor plantar on the left side, ataxic gait, scanning speech, with dysdiadochokinesis, intention tremor and dysmetria on the right upper limb. Cranial MRI, showed an infarct in the right cerebellum and right lower dorsal pons suggestive of right anterior inferior cerebellar artery infarction (Fig. 2). Discussion EFP has been characteristically associated with anterolateral thalamic infarction (tuberothalamic artery ischemia),7,8 although lesions of posterior thalamus and frontal lobe with sparing of the anterolateral thalamus have been described.2 The occurrence of EFP in the latter cases has been linked to the interruption of the connections between the thalamus and the frontal or mesial temporal lobes.2,5 These anterior fronto-thalamo-pontine connections descend in the anterior limb of the internal capsule. EFP in association with subthalamic and dorsal midbrain tumors has been attributed to the involvement of a small fibre bundle within the dorsal midbrain tegmentum.5,9 The occurrence of EFP in pontine lesions has been linked to dorsolateral pontine tegmentum infarction, conforming to the superior cerebellar artery territory.6 The uniformity with which EFP precludes classic vascular midbrain lesions like Benedikt's or Weber's syndrome as well as rostral pontine lesions is possibly linked to the ventral location of these lesions.2,10 Classically, a lesion rostral to the upper mid pons results in a contralateral supranuclear facial paresis, while ipsilateral facial paresis of the infranuclear type results from lesions of inferolateral pons.11,12 The occurrence of a supranuclear facial paresis in a lesion of the lower pons, as in our case, needs to be reckoned with. It has been hypothesized that the facial corticobulbar tract fibres may dissociate from the pyramidal tracts at the pontomedullary junction and descend caudally to atleast the middle medullary levels, before most of them cross to the opposite facial nucleus.13 The occurrence of a contralateral supranuclear facial paresis commonly results from the involvement of these descending pathways rather than the ascending pathways. Terao et al postulated that the facial CBT descend upto the upper medullary level and determined that supranucelar facial palsy was more common in lesions of lower pons and upper medulla than middle or lower medullary lesions.14 The facial CBT can thereby be considered to be constituted by looping fibres which decussate in the upper medulla. The occurrence of an ipsilateral EFP in our case, however, may be representative of the involvement of the ascending pathways. It has been deemed that the corticofacial fibres course down the mediodorsal portion of the base of pons and the volitional and emotional fibres possibly converge below the middle one-third of the pons.15 If the explanation of the ipsilateral EFP in our case holds good, it would imply that the fibres for the emotional and volitional control follow a distinct course even after their decussation. This case offers further insight into the course of the central pathways of the facial cortico-bulbar tracts. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02028f1b.jpg] [ni02028f2.jpg] [ni02028f1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}