 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
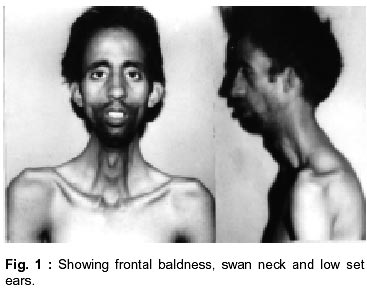
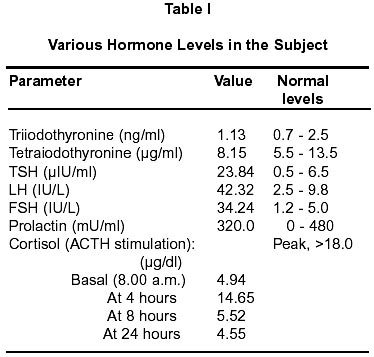
Neurology India, Vol. 50, No. 1, March, 2002, pp. 105-106 Polyglandular Endocrinopathy in Myotonic Dystrophy : Letter to Editor A.H. Zargar, M.H. Bhat, M.A. Ganie, B.A. Laway, S. R. Masoodi, M. Salahuddin,* S. Kour* Departments of Endocrinology and Immunology*, Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Kashmir. Code Number: ni02029 Myotonic dystrophy (MD) has an autosomal dominant inheritance with a high penetrance. The disease is characterized by a unique topography of muscle atrophy, myotonia and dystrophic changes in non-muscular tissues like lens of eye, testes, cerebrum, esophagus and other endocrine glands. A patient of myotonic dystrophy, who had polyglandular failure in the form of hypergonadotrophic hypogonadism, primary hypothyroidism and Addison's disease is described. A 27 year old unmarried male, first in birth order, presented to the endocrine clinic of our Institute with the complaints of anorexia, weight loss and darkening of facial features of five years duration. He also complained of weakness and stiffness of both hands and neck muscles. He could not lift his neck when in supine position. There was no history of pain abdomen, vomiting, syncope, dysphagia, or nasal regurgitation. There was no history of cold intolerance or constipation. Other sibs were normal. None of the parents had similar sickness. Clinical examination revealed a young asthenic male with buccal mucosal pigmentation and diffuse pigmentation of exposed parts of body. He had pulse of 70/minute, blood pressure of 90/70 mmHg (sitting), 80/60 mmHg (standing) and body mass index of 17.41 kg/m2. His secondary sexual characters were normal and both testes were small and atrophic. He had frontal baldness, hatchet facies, swan neck, high arched palate, low set ears, pectus excavatum and scoliosis of dorsal spine (Fig. 1). Central nervous system examination revealed normal intelligence, power grade 2-3 in neck muscles, shoulder muscles and jaw muscles. He had myotonia of the tongue and the muscles of hand. Both optic fundi were normal. Detailed investigations revealed hemoglobin of 11 gm/dl; total leucocytic count of 7500/ml (neutrophils 70%, lymphocytes 28% and eosinophils 2%) Biochemical investigations revealed normal fasting and postprandial blood sugar, normal renal and hepatic functions. Serum lactic dehydrogenase was 418 U/L (normal value 100-120); and creatine kinase, 3781 U/L (normal value 25-90). X-ray of chest, skull, hands and 12 lead electrocardiogram were normal. Semen analysis revealed azoospermia. Electromyography of deltoid showed myopathic pattern. Endocrine evaluation included estimation of trio-iodothyronine, tetra-iodothyronine, thyroid stimulating hormone, prolactin, growth hormone, and gonadotropins. ACTH stimulation test was performed with 40 units of Acthergel (a long acting preparation of ACTH) and serum cortisol levels estimated at 0h, 4h, 8h and 24h. A stimulated cortisol level of >18 µg/dl was considered normal. Details of hormone estimation are given in Table I. This patient had classical features of MD and Addison's disease. Low basal cortisol level and suboptimal elevation of cortisol after ACTH stimulation, in presence of pigmentation, hypotention and low blood glucose confirm the diagnosis of Addison's disease. Presence of small atrophic testes, elevated levels of gonadotropins and thyroid stimulating hormone confirm the diagnoses of hypergonadotropic hypogonadism and primary hypothyroidism. In patients with MD associated endocrinopathy, particularly testicular atrophy, is well documented;2,3 however, polyglandular failure is a rare phenomenon. Pizzi et al studied 12 patients with MD for any endocrine abnormalities. They documented decreased thyroid hormones in one patient. Three out of 8 patients showed no response to ACTH stimulation.4 Rioperez et al described two patients of MD, one with primary hypothyroidism and the other had non-toxic multinodular goiter.5 Pagliara et al reported hyperthyroidism and Addison's disease in a case of MD.6 An instance of isolated prolactin deficiency in association with MD has also been documented.7 Rosenberg et al published data on four patients with hyperparathyroidism associated with MD. Their data also suggests the possibility of this disorder being associated with neurofibromatosis and multiple endocrine adenomatosis type 2A. All were females aged between 2 and 45 years. They were from three separate families, with two related patients being mother and daughter.8 A recent study has documented that the total endocrine cells area in the duodenum, as demonstrated by chromogranin-A immunoreactivity, was significantly increased in MD as compared to controls. The increase included all types of endocrine cells studied, namely those positive for serotonin, cholecystokinin, gastrin, secretin, gastric inhibitory polypeptide and somatostatin. This indicates disturbed endocrine regulation of the gastrointestinal tract.9 The endocrine disturbances in MD seem to be quite varied and diverse. Our patient primarily presented with clinical features of Addison's disease. After evaluation, the concomitant presence of hypergonadotropic hypogonadism and primary hypothyroidism were confirmed. The presence of polyglandular failure, though known is rare. The high association of endocrinopathy and MD suggests possible cause and effect relationship between the two. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02029f1.jpg] [ni02029t1.jpg] |
| |||||||||

{kind=link}
{kind=link}