 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 128-135 VIEWS AND REVIEWS The Neurology of Eclampsia : Some Observations A. Chakravarty, S.D. Chakrabarti* Department of Neurology, Vivekananda
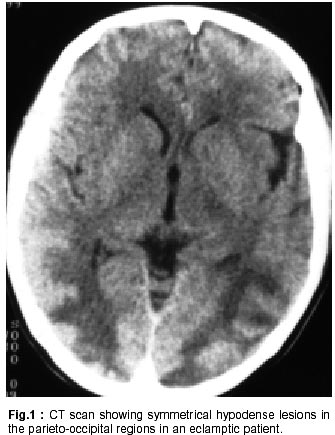
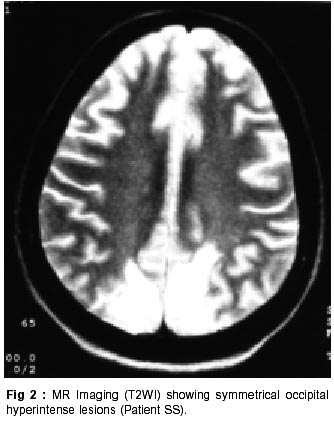
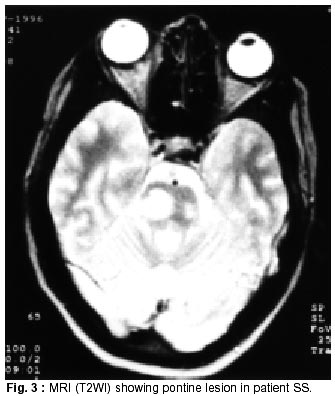
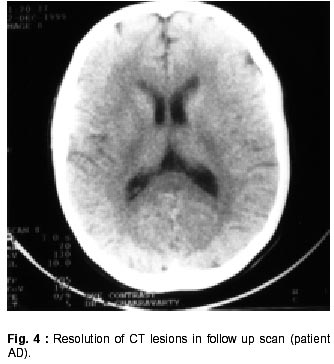
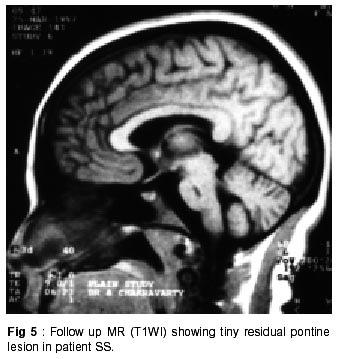
Institute of Medical Sciences and Medical College*, Calcutta -700 006, India Accepted for publication : 13th September, 2000. Code Number: ni02039 Summary Nineteen patients admitted with diagnosis of eclampsia in a large general hospital between 1996 - 1999, were analyzed. Eight patients were referred to neurologists for assessment and management. All these patients had recurrent generalized seizures. Five patients developed visual disturbance. Neuroimaging (CT and/or MRI) revealed symmetrical occipital lesions in all. One patient had a large pontine lesion. Seizure control was achieved in all with intravenous phenytoin. All patients recovered fully without any residual neurological deficit and their radiological brain lesions resolved completely, in all except one case. The neurological manifestations and neuroimaging features in cases of eclampsia have been reviewed. A brief note on the pathogenesis of the cerebral lesions is included and the controversial aspect of seizure control in eclampsia highlighted. Key words : Eclampsia, Neurologic manifestations, Visual loss, Seizure control. Introduction Pre-eclampsia is a complex disorder characterized by pregnancy induced hypertension, proteinuria and edema occurring after twenty weeks of pregnancy. The clinical presentation varies in severity and multiorgan involvement is common. The manifestations may include pulmonary edema, oliguria, disseminated intravascular coagulopathy and hepatic hemorrhages. Neurologic manifestations of pre-eclampsia include headache, confusion, hyperreflexia, visual hallucinations and blindness. Eclampsia has been defined as the occurrence of convulsion, not caused by any coincidental neurologic disease (e.g. epilepsy) in a woman whose condition also meets the criteria for pre-eclampsia.1 Preeclampsia, in effect, becomes eclampsia with the advent of a seizure or coma and would be briefly highlighted later. The cerebral lesions causing neurologic features, including seizures, presumably occur as a result of cerebral circulatory dysregulation and neuropathologic studies support this conjecture. To the best of the authors' knowledge, no comprehensive study on the neurological and neuroradiological aspect of eclampsia has been published in the current neurologic literature in India. Only a solitary case report highlighting reversible MR imaging features was reported in 1997.2 The present report describes the principal author's (AC) experience with eight patients of eclampsia, highlighting clinical neurologic aspects, neuroradiological features and seizure control measures adopted, along with a brief review of the subject. Material and Methods During the period of study, a total of 19 patients were admitted with diagnosis of eclampsia fulfilling the criteria mentioned earlier. Total obstetric admissions in the hospital during the same period had been 20,273 and total confinements were 15,411. Of these, eight cases were referred to the neurological services, principally because of recurrent seizures, prolonged alteration of sensorium, severe headache and visual loss in varying combinations. The patients were evaluated clinically several times till full recovery and were later followed up in OPD. All but one had initial CT scan of brain and three patients (including the one who did not have CT) had MR brain imaging at the initial stage. During follow-up, imaging studies were repeated between three to six months of discharge. Results General : The age range of the subjects varied from 24 to 30 years. Six were primigravida and two second gravida. None had prior history of hypertension, renal disease, diabetes or seizure disorder. All patients had been attending the antenatal clinic of the hospital and none except one showed any clinical evidence of preeclampsia upto the time of last clinic visit (3 to 4 weeks prior to admission). All were subsequently admitted with history of having had either a seizure or altered sensorium. Blood pressure on admission was over 140 mm Hg systolic and 100 mm Hg diastolic in all, with pedal edema and proteinuria. One patient had spontaneous expulsion of a dead fetus and seven underwent emergency cesarean section with only three live births. Neurologic evaluation : All patients had generalized tonic clonic recurrent seizures (3 or more over 24 hours). The seizures started prepartum in 5 and postpartum in 3 cases. At initial neurologic evaluation, all were at varying stages of altered sensorium (GCS 8-10) without any localizing sign but with hyperreflexia and bilateral extensor plantars. Six patients complained of severe holocranial headache at some stage of their illness and five complained of blurred vision either prior to losing consciousness or after improvement in level of consciousness. The visual problem in all appeared to be cortical in nature. Fundus examination revealed retinal arterial spasm in all eight patients. Four patients had diffuse retinal edema but no hemorrhages. None had any meningeal sign. Improvement in sensorium started 36-48 hours after seizure control and all were fully conscious after 72 hours. Blurred vision persisted for 5-7 days after admission in 5 patients who had this symptom. Neurologic management : All patients were prescribed methyldopa by their obstetricians for control of hypertension and one needed intravenous infusion of glyceryl trinitrate. Obstetricians also put all patients on diazepam infusion (20-30 mg over 12 hrs.) but seizures persisted inspite of this. No patient was given magnesium sulphate. Seizure control in 8 patients referred to the neurologists was achieved with intravenous phenytoin, using a similar protocol as practiced in status epilepticus but at a slower rate. Phenytoin 15 mg/kg was given by infusion pump over 60 minutes and was followed by bolus injections of 100 mg intravenous every 6 hours for 48 hours and thereafter oral therapy was instituted. No patient had breakthrough seizures. In addition, intravenous infusion of mannitol was given intermittently in the first 48 hours. At the time of discharge (10-14 days after admission), no patient had any residual neurologic sign or symptom. Oral phenytoin was continued for 3 months after discharge. Neuroradiological evaluation : CT scan of brain was done within 48 hours after admission in seven patients. All showed bilateral symmetrical occipital hypodense lesions involving more of white matter than the grey. In five patients, lesions extended to the parieto-temporal areas of both sides (Fig. 1) but never extended anteriorly beyond the sylvian fissure. No lesions could be detected in the brain stem or in the basal ganglionic regions. Areas of hyperdensity within the hypodense areas (suggesting hemorrhages) were seen in 3 patients. MR study could be done early in 3 cases only, including one case where CT was not done. The lesions corroborated well with the CT findings. Hypointense lesions on T1WI and hyperintense lesions on T2WI and proton/flare sequences were seen symmetrically in both occipital regions with some extension in the parietotemporal regions (Fig. 2). The lesion involved more of white than grey matter. In one case, small hyperintense lesions were seen on T2WI and proton density images in posterior limb of internal capsule, both thalami and subcortical white matter of right frontal lobe. The pons also revealed hyperintense lesion on T2WI (Fig. 3) and proton density images, with the larger lesion in right paramedian aspect. The latter lesion most likely represented an area of hemorrhage. MR angiographic studies were not done in any patient. Follow up neuroradiological evaluation : Seven patients had follow up contrast CT scan of brain, 3-4 months after discharge. Neurologically, all were normal with normal blood pressure, without any medication. The repeat scan did not show any evidence of the lesions detected earlier (Fig. 4). This suggested that the earlier hypodense lesions were most likely areas of edema rather than infarction. The hemorrhagic areas also resolved completely. The single case with pontine lesion had a repeat MR scan 6 months later. While all the cerebral lesions completely resolved, a tiny area of hypointensity on T1WI (Fig. 5) and hyperintensity in T2WI persisted in the pons, suggesting presence of either a small infarct or a posthemorrhagic gliotic area. She was clinically asymptomatic and had no residual neurologic signs. Discussion Pathogenesis and cerebral pathology : Preeclampsia/ eclampsia is now considered to be primarily a placental disorder. Both poor placentation as well as hyper-placentosis (e.g. twins/molar pregnancies) are associated with this condition.3 It is believed that either an unknown factor (factor X, as some call it) or villous debris from the malformed placenta manage to reach the maternal circulation, eliciting an immunological response from the mother's system.4 Other variables like dietary factors, namely protein and caloric deficiency, lack of essential fatty acids, deficiency of magnesium, calcium, zinc and an excess of sodium as well as genetic factors like abnormal alleles for the genes of TNF-a, angiotensinogen, factor V and nitric oxide synthase (NOS) predispose to this event.5-8 The maternal response is primarily immunological with increased activation and functional abnormalities of maternal neutrophils, high circulating levels of the cell-adhesion molecule VCAM-1 (which helps to mediate neutrophil activity) and occurrence of immune-complexes in the placenta, maternal serum and various organs.9,10 The effect of this maternal response is widespread cellular dysfunction with multi-system involvement.11 There is endothelial damage with increased capillary permeability, raised fibronectin levels and electron microscopic evidence of damaged endothelium.12,13 Coagulation abnormalities occur, caused by increased activation and consumption of platelets, low antithrombin III levels, abnormal prostaglandin metabolism and in a few cases, florid DIC.13,14 Endocrine anomalies include activation of the renin-angiotensinaldosterone axis, abnormal catecholamines and abnormalities in progesterone metabolism.13 These pathophysiological changes lead to hypertension, edema, proteinuria, bleeding tendencies, renal dysfunction, liver damage and the neurological abnormalities. Neurological effects of pre-eclampsia/eclampsia can be antepartum or post-partum, the latter being more common.15 These are due to irregularities in the autoregulation of cerebral circulation.16 Disruption of the blood-brain barrier occurs due to both the hypertension-induced capillary damage and the immune-mediated endothelial dysfunction. This leads to extravasation of red cells and plasma proteins into perivascular space causing cerebral edema.17 Cerebral vasospasm, produced by a combination of reaction to hypertension, prostaglandin deficiency, defects in the e-NOS gene (coding for nitric oxide systhase) and endothelial damage, play an important role, producing ischemia and infarction in the brain tissue.18-19 The impaired blood coagulation system and the abnormalities and deficiency of platelets predispose to intra-cranial bleeds.20 Thus, a varied picture of cerebral pathology, showing evidences of cerebral edema, micro-infarcts, cortical petechiae and pericapillary hemorrhages is observed in the brains of patients with pre-eclampsia or eclampsia, which clinically manifest as headache, visual disturbances, confusion and seizures. Neurologic features : The hallmark of eclampsia is onset of seizures, which may be focal motor or generalised tonic clonic. As indicated earlier, they may appear before, during or after childbirth but usually within first 24 hours postpartum. Delayed onset of seizures has also been reported.21 In the present series, however, seizure onset was more prepartum (5 cases) than postpartum (3 cases). This need not necessarily represent the general pattern as only selected cases referred to neurologists were included. All had generalised tonic clonic seizures. None of the patients had any focal neurologic deficit though all had bilateral symmetrical pyramidal signs. Vision related symptoms are well recognised in eclampsia.22 Retinal arterial dilatation, papilledema, angiospasm, occlusion of central artery, hemorrhages, exudates and edema - all have been described. While all 8 cases in the present series had angiospam and 4 had retinal edema, none had papilledema, hemorrhages or exudates on fundoscopy. The blurred vision complained by 5 subjects was thought to be of central origin and was corroborated with imaging features of bilateral occipital involvement. Affection of the posterior part of visual pathway has been well recognized.22-26 The visual cortex was affected by edema, micro-infarctions and microhemorrhages in all patients in the present series. Visual symptoms, of course, normalised in all in a few days time. Neuroimaging in severe pre-eclampsia/eclampsia : The pathological features described earlier were reflected in the neuroimaging features seen in the present series. CT scan in eclampsia patients revealed a wide spectrum of findings ranging from normal to focal occipital or more widespread lesions which were hypodense and non-enhancing and were ascribed to localised edema.27 Repeat CT has shown partial or complete resolution within 2 weeks. Cerebral hemorrhage including subarachnoid hemorrhage has also been described.28 A number of MR studies confirm the presence of hyperintense lesions on T2WI in eclampsia.29-31 Commonly, these have been found in the posterior circulation territory with involvement of cortical and subcortical white matter in occipital and posterior parietal lobes. These lesions are bilaterally symmetrical and follow the gyri in a serpentine manner. Lesions have been described in the deep white matter and basal ganglionic areas, which are hyperintense in long TR images but occasionally also in T1WI, suggesting microhemorrhages. Almost all such lesions were transient, suggesting the development of edema due to failure of autoregulatory mechanism or transient vasospasm. Reversible cerebral vasospasm by MR angiography has recently been described in pre-eclampsia.32 On the other hand, cerebral blood flow measured by SPECT in one patient during an attack of visual disturbance showed increased blood flow in the occipital cortex.33 The combination of vasodilatation and vasospams in the pathogenesis of ecalmpsia has already been commented upon in the section on pathogenesis. CT and MRI findings in the present series corroborated with those described earlier. On CT scanning, the lesions never extended anteriorly, but frontal white matter lesions could be detected on MRI. Similarly, central grey matter lesions were more apparent on MRI than on CT scan. The observation of pontine lesion on MRI in one subject, though she never developed any classical pontine clinical syndrome, was interesting. Such brain stem lesions have not been highlighted in earlier studies. This was also the only case in the present series where a tiny residual abnormality presisted on repeat scanning after 6 monhts. MRI, indeed, gives more accurate assessment of the degree of CNS involvement in eclampsia. Seizure control in eclampsia : All eight patients in the present series had been treated with intravenous phenytoin (PHT) with initial loading dosage, followed by intermittent intravenous bolus doses over next 48 hours. No doubt, some eyebrows would be raised in this regard especially among obstetric colleagues. Although five of the eight patients in this series had antepartum onset of seizure, by the time they were seen by the neurologists, one already had spontaneous expulsion of the fetus and the rest 7 had emergency cesarean section done. Attempt at initial seizure control was made by the obstetricians with intravenous diazepam and no patients received magnesium sulfate (MgSO4 ). PHT was resorted to later after neurologic referral, either for control of ongoing seizure or prevention of further seizure. PHT proved to be successful in this regard and no maternal complications in the postpartum period could be attributed to PHT therapy. There is a lot of controversy in the literature and in medical practice about the choice of anticonvulsants in eclampsia. An ideal anticonvulsant should have good seizure control, should not affect uterine function, should lower overall maternal morbidity and mortality and should not affect fetal morbidity or mortality, if used antepartum. It is also important to consider whether the drug has been used during the stage of preeclamspia to prevent onset of seizures or during eclamptic phase to control seizures. These issues need to be carefully judged and remembered while examining the results of several trials done in recent times. Rapid control of a single seizure episode can certainly be achieved with a bolus dose of diazepam. The efficacy of intravenous infusion in preventing seizure recurrence is doubtful and repeated bolus injections not usually practiced in pregnancy for its possible adverse effects on the fetus e.g. hypotonia, hypothermia, apnea etc.34 The need, therefore, is for a longer acting drug and MgSO4 and PHT seem to be the main contenders. Most obstetricians all over the world probably still use MgSO4 both in pre-eclampsia to prevent seizures and in eclampsia to control and prevent recurrence of seizures. Mechanism of action is not clearly known. This may involve blockade of NMDA receptors involved in seizure genesis35 or calcium channel blocking, preventing cerebral vasospasm.36 MgSO4 , in experimental seizure models, does not appear to have a very significant anticonvulsant action37,38 and certainly is not a standard anticonvulsant for treatment of epileptic seizures. A closer look at available recent literature would however suggest, that more emphasis has been given to prevention of seizures in pre-eclampsia, with MgSO4 , than actual rapid seizure control and preventation of recurrent seizures. There are also problems associated with MgSO4 including local irritant effect, loss of patellar reflex (a common sign used by many obstericians in this country to check for toxicity), lethargy and depression in mother and newborn and recurrence/refractoriness of seizures in many.39,40 From neurologists' stand point, rapid control of seizures and preventing its recurrence needs to be achieved with a time tested proper anticonvulsant e.g. phenytoin. This view is gradually being shared by obstetricians as well. The efficacy of PHT in controlling eclamptic seizure was probably first reported by Slater et al in 198741 and subsequently several reports were published in the first half of 1990s.42 Some early reports on breakthrough seizures were probably related to low therapeutic level achieved. The dosage schedule is similar to that used in status epilepticus, but given at a slower rate, preferably with checking of serum levels from time to time (difficult to perform in our setting and not done in any case in the present series). Other dosage regimes have also been suggested. A single high dose intravenous PHT (900 mg) had been used with success in patients with eclampsia, given on admission, with no untoward effects in the mother and the neonate.43 A study in a premier obstetric hospital in U.K. compared different loading doses of PHT and preferred a dosage of 15 mg/kg and stressed the need to follow it up with boosting doses to maintain therapeutic plasma level.44 Occasionally, however, seizures recurred even with serum PHT level well within the therapeutic range. Quite a few controlled trials in recent times have tried to establish the efficacy MgSO4 over PHT. Lucas et al45 randomised over 1000 patients with pregnancy induced hypertension and pre-eclampsia to receive either drug and concluded that MgSO4 is superior to PHT in preventing eclampsia (the two groups being comparable regarding the risk). Naidu et al46 used transcranial doppler (TCD) to assess degree of cerebral vasospasm in eclamptic patients receiving either MgSO4 or PHT. MgSO4 significantly reduced the pulsatality index and mean flow velocity compared to PHT in the middle cerebral artery and thus appeared to be a better drug to reverse cerebral vasospasm, a major factor implicated in the pathogenesis of eclampsia. Chien et al47 tried to establish the efficacy of MgSO4 from retrospective analysis of randomised trials through online search of Medline database between 1966-1995. 1743 patients with pre-eclampsia included in nine randomised trials were assessed for seizure activity and maternal death. On both the scores, MgSO4 was favoured as compared to PHT and the authors concluded MgSO4 to be a superior drug compared to PHT in preventing seizures in eclampsia and seizure prophylaxis in preeclampsia. A recent Indian study48 randomly allocated 50 pregnant women with eclampsia to receive either MgSO4 or PHT. Women treated with PHT had a higher incidence of recurrent seizures but perinatal mortality and morbidity and maternal mortality were comparable in both groups. The most recent data is available from the Cochrane database system review.49 Four well controlled trials encompassing 823 women were included. MgSO4 (as compared with PHT) was associated with a substantial reduction of recurrence of seizures, a favourable trend in maternal mortality, reduction in risk of pneumonia, ventilation and admission in ICU of mother and admission of babies in special care units and reduction in perinatal mortality. All these favoured use of MgSO4 compared to PHT. A close look at the forementioned trials would bring forth a few important points. In the eye of a neurologist, PHT is a proper well-tested anticonvulsant and not MgSO4 . But the latter appears to have some 'disease modifying' effect in the setting of toxemia of pregnancy. Hence, in a patient admitted with seizures, ideal treatment would be control of the seizures first using a loading dose of proper anticonvulsant like PHT and supplementary therapy with MgSO4 may provide added benefit in preventing recurrence of seizures and inproving maternal and perinatal mortality or morbidity. On the other hand, in patients admitted with severe pregnancy induced hypertension and pre-eclampsia, MgSO4 would undoubtedly be the drug of choice for preventing onset of seizures and reducing morbidity and mortality. In the present series, PHT was used in all patients, as all presented with recurrent seizures and rapid seizure control deemed mandatory. Furthermore, as neurologists, we were more accustomed to use PHT than MgSO4 . No clear guideline is given anywhere for the duration of anticonvulsant therapy in eclampsia. In the present series, oral anticonvulsants were continued for 3 months postpartum, based only on the observation that the radiological resolution of the CNS lesions (discussed earlier) occured in about 3 months. It is felt that management of eclampsia and severe preeclampsia must be made through close liaison between the obstetricians and the neurologists. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02039f4.jpg] [ni02039f2.jpg] [ni02039f1.jpg] [ni02039f3.jpg] [ni02039f5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}