 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 136-140 Transsphenoidal Line of Vision on MRI for Pituitary Tumor Surgery A.G. Chacko, M.J. Chandy Department of Neurosurgery, Christian Medical College and Hospital, Vellore
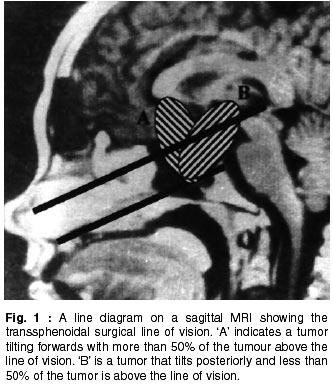
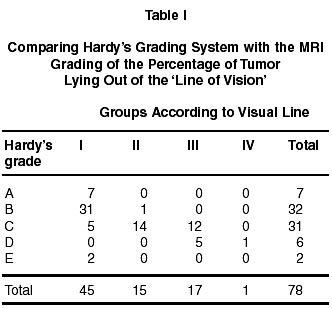
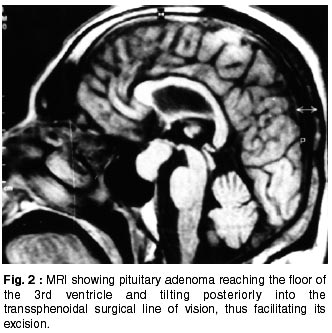
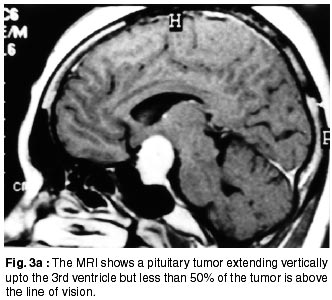
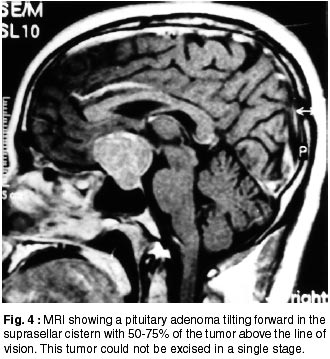
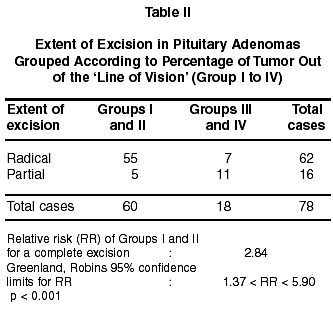
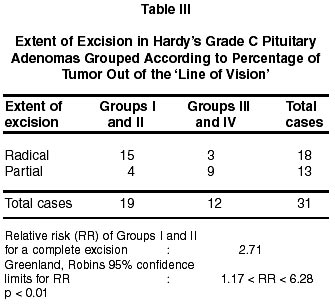
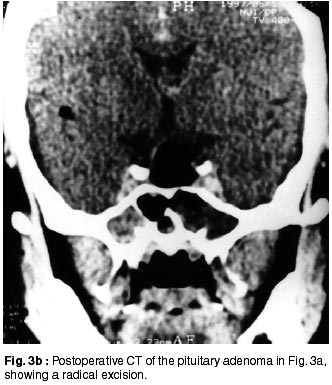
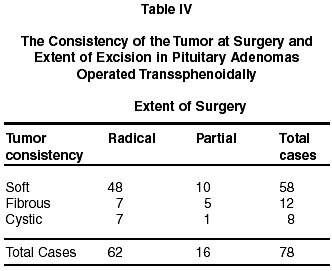
- 632 004, India. Accepted for publication : 20th March, 2001. Code Number: ni02040 Summary This study was done to determine the usefulness of the sagittal magnetic resonance image (MRI) in predicting the ease of resectability of pituitary adenomas operated through the transsphenoidal route. Tumors were graded according to Hardy's method and a new system proposed by us. In this system the amount of tumor above the line of vision (V-line) as seen on the sagittal MRI was estimated and correlated with the extent of excision assessed on the postoperative computed tomogram (CT). There were 7 Hardy's grade A (8.8%), 32 grade B (41.3%), 31 grade C (37.5%), 6 grade D (8.8%) and 2 grade E tumors (3.8%) among the 78 tumors studied. It was seen that most of the tumor volume was below the V-line in Hardy's grade A and B tumors. In grade C tumors 5 were < 25% above, 14 were 25-50% above and 12 were 50-75% above the V-line. A radical excision was possible in 15 of l9 grade C tumors in which < 50% of the tumor was above the V-line. However, only 5 of 12 with Hardy's grade C were radically excised when >50% of the tumor was above the V-line. In conclusion, Hardy's grade C tumors are not a homogenous group radiologically and using the V-line on MRI helps in predicting the case of respectability in a single stage. Key words : Transsphenoidal surgery, Pituitary adenomas, MRI. Introduction Radical excision of the tumor with restoration of vision and preservation of pituitary function are the goals of surgery for pituitary adenomas. The transsphenoidal approach fulfills these goals with minimal morbidity and mortality.1 The size of the adenoma is an important factor determining the extent of excision, the ease of resectability, biochemical cure and the incidence of complications.2-4 Hardy's classification of the suprasellar extension of pituitary adenomas5,6 uses the relationship of the superior capsule of the tumor with the 3rd ventricle and takes into account asymmetric extension in the coronal plane (Grade D tumors). Grade C and D tumors are considered difficult to excise, however, it is possible to remove some of these tumors radically through the transsphenoidal route.6,7 We analyzed the sagittal MRI scans of pituitary macroadenomas to determine whether the transsphenoidal surgical line of vision helped in assessing the ease of resectability of these tumors. Material and Methods 176 patients were operated upon for pituitary adenomas via the transsphenoidal route between January 1994 and September 1996, at the Christian Medical College Hospital, Vellore, India. Patients with microadenomas and those without preoperative MRI scans were excluded from the study. There were 78 transsphenoidal procedures in the 76 patients who fulfilled the inclusion criteria, two patients having undergone second stage surgeries for residual tumor. There were 48 male and 28 females, with ages ranging from l8 to 67 years. There were 11 growth hormone (GH) secreting tumors, 14 prolactinomas (PRL), 48 non-functional and 3 mixed GH-PRL tumors. Radiological grading of tumors : Tumors were graded by a modification of Hardy's method from A to E. Using the preoperative sagittal MRI, the tumors were also graded by a new method proposed by us. The transsphenoidal surgical line of vision was drawn on a mid-sagittal MRI scan in the following manner: the anterior end of the hard palate was joined to the posterior end of the floor of the sella by a straight line. At the level of the tuberculum sellae, another line was drawn parallel to the first and extended posteriorly (Fig. 1). The tumor above the second line was therefore out of the line of vision and was expressed as a percentage of the tumor on that MR slice. The cases were divided into 4 groups, Group 1 = < 25% above the line of vision, Group 2 = 25-50% above, Group 3 = 50-75% above and Group 4 = > 75% above the line of vision. Operative techniques : After general anesthesia a lumbar subarachnoid catheter was placed in all patients for saline infusion, intracranial pressure monitoring and determination of the cerebral perfusion pressure. All patients were operated via the transnasal, transsphenoidal route. Upon entering the sphenoid sinus the image intensifier was used to identify the sellar floor. The latter was opened until the intercavernous sinus was seen anteriorly. The dura was opened in a rectangular fashion, dissection begun along the floor of the sella and along the dorsum sellae and then continued along the cavernous sinus on both sides. The suprasellar portion of the tumor was progressively brought into the line of vision by gentle traction and lumbar subarachnoid infusion of saline.8 The arachnoid that descended anteriorly and posteriorly was dissected from the superior capsule. If the field was obscured by the arachnoid pouch, removal of cerebrospinal fluid from the subarachnoid catheter lowered the intracranial pressure and raised the arachnoid. If the tumor was excessively fibrous or did not descend adequately into the line of vision, the surgery was restricted to a partial excision. The excision was considered radical when a contrast CT scan on the 7th postoperative day showed no tumor. Results Comparing Hardy's grading and the transsphenoidal line of vision (Table I) : Hardy's Grade A, B and E tumors were mostly within the line of vision, corresponding to Group I in our classification. However, Grade C tumors were not a homogeneous group. There were five tumors that tilted posteriorly in the suprasellar compartment with < 25% of the tumor out of the line of vision (Fig. 2). Fourteen tumors extended vertically in the sagittal plane with 25-50% of the tumor above the line of vision (Fig. 3a). Finally there were 12 tumors that tilted anteriorly resulting in > 50% of the tumor lying outside the line of vision (Fig. 4). The transsphenoidal line of vision and extent of excision: Table II shows a single-table analysis of the grading according to the line of vision and the extent of excision. For the statistical analysis, groups I and II, comprising cases that had <50% of the tumor out of the line of vision, were taken together and groups III and IV, that had >50% out of the line of vision were combined. The chances of excising a tumor radically was almost twice as high in Groups I and II compared with groups III and IV. (p<0.001). On analyzing Hardy's grade C tumors alone (Table III), it was found that 15 of 19 tumors in groups I and II were radically excised (Fig. 3b), while only 4 had partial excisions. On the other hand, only 3 of 12 (25%) tumors in groups III and IV had radical excisions while 9 (75%) were partially excised. (Greenland, Robins 95% confidence limits for RR 1.17 < RR < 6.28 ; p<0.01). Tumor consistency (Table IV) : On considering the consistency of the 78 tumors, 12 were fibrous, 5 (42%) of which were partially excised and the remaining were biopsied. Forty eight (82.5%) of the 58 soft tumors were radically removed. Discussion In the surgical management of pituitary macroadenomas the transsphenoidal approach has become the preferred operation because of its low morbidity and mortality.2,3,5-7,9 The factors determining a complete excision are cavernous sinus invasion, size and consistency of the tumor. Several authors2,5 have looked at cavernous sinus invasion or parasellar extension as a reason for an incomplete excision. Hashimoto et al6 and Saito et al10 discussed the fibrous or woody nature of some pituitary tumors that had large quantities of connective tissue and the difficulty in bringing them down into the sella. On the other hand, soft tumors and those containing fluid lend themselves to a radical excision independent of their size. Unfortunately, the consistency and vascularity of the tumors cannot be predicted reliably on the MRI scan unless there is blood or a cyst. Mohr and Hardy classified the suprasellar extension of pituitary macroadenomas based on a coronal CT scan and measured the vertical height of the tumor above the jugum sphenoidale.3 The grade A and B tumors were considered easier to excise while the removal of grade C and D tumors, those that had a superior margin more than 20 mm above the jugum sphenoidale, was more difficult (40% had residual tumor on the postoperative CT scan). The coronal images provided additional information regarding asymmetric lateral expansion of the tumor (grade D) that made a complete excision technically more difficult. Wilson's modification of Hardy's system11 introduced a 'stage E' when there was a direct lateral extension into the cavernous sinus and subsets to the 'stage D' when there was extension into the anterior, middle and posterior fossae. We focussed our attention on the sagittal MRI scans to determine additional features that would help in preoperative planning. Our hypothesis was that given the limitation of a narrow and deep operating field during a transsphenoidal surgery, the amount of tumor lying out of the line of vision would be an important factor determining the case of resectability and completeness of excision. Although it is possible to alter the position of the Hardy's speculum and angle the microscope anteriorly to obtain a wider field of view, we used the straight line of vision for an objective assessment. We found that when <50% of the tumor was above the line of vision the chances of a radical excision was significantly higher than when >50% was above the line of vision. Furthermore, Hardy's Grade C tumors are not a homogeneous group radiologically. About 16% of Grade C tumors tend to tilt posteriorly into the transsphenoidal line of vision and are more easily excised than the remaining 40% that tend to tilt anteriorly growing out of the transsphenoidal line of vision. Recent reports suggest that transsphenoidal endoscopic pituitary surgery is useful in selected pituitary adenomas.12,13 Although visualization is improved, its efficacy in the safe removal of large tumors out of the transsphenoidal line of vision remains to be seen. In conclusion, the transsphenoidal surgical line of vision on a sagittal MRI is useful in assessing the ease of resectability of pituitary adenomas, especially in Grade C tumors. Depending on the clinical course, it may be possible to plan either a second stage transsphenoidal surgery or a craniotomy when more than 50% of the tumor is above the line of vision. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02040t1.jpg] [ni02040t4.jpg] [ni02040f2.jpg] [ni02040f1.jpg] [ni02040t3.jpg] [ni02040f3a.jpg] [ni02040f3b.jpg] [ni02040t2.jpg] [ni02040f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}