 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 141-144 Acute Symptomatic Seizures Due to Single CT Lesions : How Long to Treat with Antiepileptic Drugs ? A. Thussu, A. Arora, S. Prabhakar, V. Lal, C.P. Das, I.M.S. Sawhney Department of Neurology, Postgraduate Institute of Medical Education and Research,
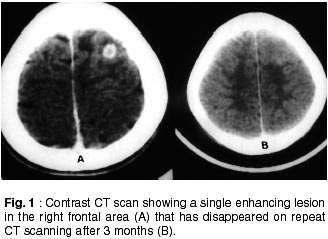
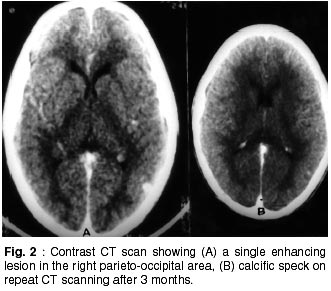
Chandigarh-160012, India. Accepted for publication : 22nd August, 2001. Code Number: ni02041 Summary The duration of anti epileptic drug therapy for single small enhancing CT lesions (SSECTL) presents a major dilemma. We studied the efficacy of short duration (6 months) antiepileptic drug therapy as compared to long duration (2 years) drug therapy. Seventy three patients presenting with seizures and showing SSECTL on cranial CT scans (plain and contrast) were randomized into group A (6 months therapy) and group B (2 years therapy). There were 47 patients in group A and 26 patients in group B. Patients were followed up for one year after withdrawal of anti epileptic drugs. CT Head (plain and contrast) was repeated after 3 months, or earlier in cases of recurrence to rule out reinfection. 53.2% in group A and 53.8% in group B showed complete resolution and were seizure free on one year follow up. Punctate residual calcification was seen in 46.8% in group A and 46.2% in group B. Eight patients (17%) in group A and three (11.5%) in group B had a recurrence. The difference in recurrence of seizure between the two groups was not statistically significant (p<0.77) in the calcified lesion subset. Since none of the patients in total resolution subset showed recurrence, the difference between calcified and total resolution subset was highly significant. The study shows that a short duration (6 months) AED therapy in patients with total resolution of lesion on follow up scan, may be adequate in comparison to those who have calcific speck as a residue. However, a longer duration of therapy in case of calcific group probably does not alter their chances of recurrence. Key words : Single CT Lesions , Cysticercosis, Symptomatic seizures. Introduction Single small enhancing CT lesions (SSECTL) are a common finding on cranial CT of Indian patients presenting with seizures.1-2 These have also been occasionally reported from many other countries including Australia, U.K., U.S.A., Hong Kong, Thailand, Belgium, Portugal and South Africa. Similar lesions have also been labelled as 'acute lesion' by some authors.3-9 Bhargava and Tandon10 were the first to draw attention towards this entity in Indian patients having epilepsy. Etiologic possibilities earlier considered for this entity include tuberculosis, focal encephalitis, microabscesses and cysticercosis. But current opinion favours cysticercosis as being the most plausible cause. The lesion undergoes either spontaneous resolution or calcifies with passage of time. The duration of antiepileptic drug therapy in these patients has not been clearly worked out and neurologists favor an epileptic regimen for two years or more, as for idiopathic epilepsy. The present study was undertaken to compare the results of short duration (6 months) antiepileptic therapy with long duration (2 years) antiepileptic drug therapy in patients presenting with SSECTL. Material and Methods The present study included patients presenting to the neurology out patient of the Postgraduate Institute of Medical Education and Research, Chandigarh, in a two year period. Seventy three patients presenting with seizures, who showed SSECTL on a contrast enhanced CT scan (ring enhancing/disc lesions, < 20 mm in size) were enrolled. The enrolled patients had their first seizure within one month of their entry into the study. None of the patients had long-standing epilepsy. A complete history regarding the type and frequency of seizures, presence of Todd's palsy, headache and any other symptoms were recorded at presentation. Patients were subjected to Mantoux test, X-ray chest (PA view), cysticercus serology and EEG. Stool test for ova and cysts of parasites was carried out in all cases. A repeat plain and contrast enhanced CT scan was done on follow up at 12 weeks. In some patients, there was total disappearance of the lesion (Fig. 1). In others, there was a punctate calcified residua (Fig. 2). Cases who had persistence of the lesion, were put on albendazole and excluded from the study. Patients were allocated into two groups with simple random sampling technique using lottery system. Patients in group A were given antiepileptic medication for 6 months and then tapered over the next 3 months. Patients in group B were given antiepileptic therapy for a period of 2 years which was tapered over next 3 months. Patients were informed about the nature of the study at the time of inclusion into the study and informed consent was taken. Both the groups were kept on two monthly follow up after cessation of antiepileptic therapy, for one year to detect possible recurrence of seizures. All recurrences were documented, based on clinical history taken independently by two observers. In case of conflicting views regarding epileptic/nonepileptic nature of the event, views of a third observer were taken as final. CT head (plain and contrast) was repeated to rule out reinfection, in cases who had recurrence of seizures. Statistical analysis of the data available was done using chi square test. 'p value' of less than 0.05 was considered significant. Results The study included 73 patients, 47 in group A and 26 in group B. Since the study was done in a fixed time frame and strict randomization was done, the two groups got unequal number of patients. Group A : Out of 47 patients in group A, 22 were males and 25 females. The average age was 19.5+8.79 years (age range 4-46 years). Twelve patients had simple partial seizures, 22 had partial motor seizures becoming secondarily generalized, while 13 presented with generalized seizures. Only one patient had a focal neurological deficit after partial motor seizures, which subsequently improved. Twelve patients had disc lesion on CT scan while 35 had ring-enhancing lesions. On follow up CT, 25 patients (53.2%) showed a complete resolution of lesion while 22 (46.8%) patients showed residual punctate calcification. X-ray chest was done in all 47 patients and was normal in all. Cysticercus serology was done in all the cases but was positive only in 8 (17%). Mantoux test was positive in only 4 patients out of 47. Stool examination did not reveal ova of Taenia solium in any patient. 25 patients were treated with carbamazepine and 22 with phenytoin. The choice of drugs depended upon the affordability of drugs by the patients. None of the patiens had a seizure recurrence after achieving the therapeutic dosage of the given drug according to weight. Patients were given antiepileptic therapy for 6 months which was tapered off over the next 3 months. Group B : Group B comprised of 26 patients, 17 males and 9 females. Mean age of the patients was 25.6+12.5 years (age range 10-52 years). Twenty six patients presented with partial motor seizures becoming secondarily generalized, 6 with simple partial motor seizures and 6 with generalized tonic clonic seizures. Post ictal neurological deficit was present in 3 patients on presentation, which subsequently resolved without any specific therapy or antiedema measures. CT scan showed a ringenhancing lesion in 18 (69.2%) patients while 8 (30.8%) showed disc lesions on CT scan. Fourteen (53.8%) patients showed complete resolution of lesion on CT after 3 months, while 12 patients (46.2%) showed punctate calcification. Cysticercus serology, done in all 26 patients, was positive only in 2 patients (7.7%). X-ray chest was normal in all the patients of the study group. Mantoux test was positive in 3 (11.5%) patients. Thirteen patients were put on carbamazepine and 13 were on phenytoin. All patients were seizure free after achieving therapeutic dosage according to weight. Patients were given antiepileptic drugs for a period of two years and then drugs were tapered off over the next 3 months. Patients were followed up for one year after withdrawl of antiepileptic therapy for a possible recurrence. Recurrences : Eight cases (17%) in group A showed recurrence of seizures as compared to 3 cases (11.5%) in group B. The difference in recurrence between the two groups was not statistically significant (p<0.77). All these 11 cases with recurrence belonged to the group of 34 patients with a calcific residue on cranial CT scans at the end of 3 months. There was no recurrence in those cases where cranial CT was normal at the end of 3 months in both the groups. Thus, no comparative data can be derived from this group of patients. Discussion SSECTL is an important cause of acute symptomatic seizures in India. Wadia et al1 reported 39 patients (26%) with SSECTL out of a total of 150 patients of partial seizures. A lot has been discussed about the nature of such lesions and well-established criteria for diagnosis have been laid down. Majority of the lesions are thought to be because of cysticercosis.11 In the present study, cysticercosis is the probable etiology in majority of cases, since none of the patients had evidence of other postulated etiologies. None of the patients showed an increase in size of the lesion on follow up. Patients with persisting lesion on follow up were excluded from the study. There are no reports about antiepileptic drug management (AED) of such cases. Chandy et al12 have discussed an overall approach to the management of patients having SSECTL but they remain silent about the duration of antiepileptic drug treatment. The results of the present study suggest that one group of patients shows complete resolution while the other showed a residual punctate calcification. In other studies, a third group has been shown to retain the same size or show mild reduction in the size of lesion at the end of three months.13-14 Magnetization transfer spin echo (MTSE) MRI has been shown to detect perilesional gliosis in some cases where conventional spin echo MRI showed clearance of lesion.15,16 Hence, the disappearance of lesion by conventional imaging may not be a genuine clearance in some cases. However, this is outside the purview of the present study. In the present study, patients who had a normal contrast enhanced CT scan at 12 weeks follow up, did not show any recurrence even when drugs were tapered after 6 months of AED therapy. A longer duration of therapy is not warranted in such cases. Murthy et al expressed similar views in a retrospective analysis of 102 patients.17 In their study, only one patient had a relapse and in that case a follow up cranial CT showed a gliotic scar at the site of previous lesion. They concluded that epilepsy associated into SSECTL is a benign form of epilepsy and seizures occur as long as the lesion persists. However, patients in whom a calcific speck persisted had a greater chance of recurrence. High frequency of recurrence after AED withdrawl (50%) has also been reported in patients of neurocysticercosis with single and multiple lesions.18 The development of parenchymal brain calcification is an important risk factor for recurrence of seizure after AED withdrawl. The present study shares a similar conclusion, but as the former study comprised of a heterogenous group of neurocysticercosis and not just single CT lesions, the frequency of recurrence was higher. Moreover, our numbers are too small for deriving definitive conclusions. A comparison between short duration (6 months) and long duration (2 years) treatment for calcific lesions that had no recurrene of seizures, did not achieve statistical significance. These cases tend to have a high frequency of seizure recurrence and the duration of AED treatment in these cases is conjectural at present. The adequate duration of treatment in such cases is an individual prerogative of the physician. Since patients in the group with complete resolution on follow up did not have a seizure recurrence, what needs to be further worked out is whether the treatment duration of six months is the sacrosanct limit or the treatment duration can be further shortened. References
The following images related to this document are available:Photo images[ni02041f1.jpg] [ni02041f2.jpg] |
| |||||||||

{kind=link}
{kind=link}