 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 145-147 Randomized Prospective Study of Outcome of Short Term Antiepileptic Treatment in Small Single Enhancing CT Lesion in Brain M. Gupta, P. Agarwal, G.A. Khwaja, D. Chowdhury, B.Sharma, J. Bansal, S. Anand Department of Neurology, G.B. Pant Hospital, New
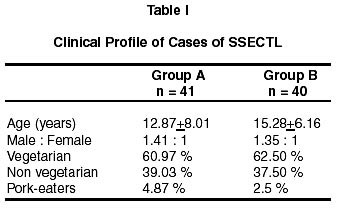
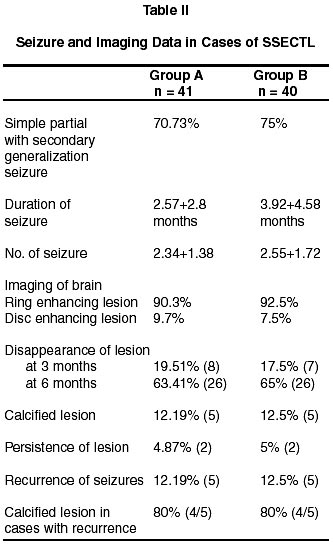
Delhi - 110 002, India. Accepted for publication: 30th November, 2001. Code Number: ni02042 Summary The study was conducted in 81 patients of epilepsy with small single enhancing CT (SSECT) lesion in brain to determine the clinical profile and duration of antiepileptic drugs (AEDs) treatment. The patients were randomly divided into group A (41 cases) and group B (40 cases). Group A patients were treated for 6 months and group B for 1 year with AEDS without cysticidal drugs. The most common mode of presentation was simple partial motor seizures with secondary generalization in both the groups. Repeat imaging of brain (CT/MRI) at 6 months showed disappearance of lesion in 82.94% in group A and 87% in group B, while persistence of lesion was present only in 4.87% in group A and 5% in group B. 87.81% patients in group A and 87.17% in group B were seizure free. The recurrence of seizure occurred in 12.19% cases in group A, and 12.82% in group B. 80% of these patients had calcified lesion in both the groups. This study reveals that SSECT lesion with epilpesy is a benign self-limiting disease. It also reveals that 6 months AED treatment is as effective as one year treatment. Patients having calcified lesion or persistence of lesion might require long term AED treatment. Key words : SSECT, CT, Epilepsy, Antiepileptic drugs, Neurocysticercosis. Introduction Small single enhancing CT lesion (SSECT) in the brain is the commonest cause of epilepsy in India . It accounts for 8% of total seizures and 26% of focal seizures in India.1,2 Initially, there was much speculation regarding the etiology of SSECT.2-6 Later on, it was found that neurocysticercosis (NCC) was the commonest cause of SSECT lesion, other etiologies being tuberculomas and non specific inflammation.6 Now it is an established fact that SSECTL with seizures is a self-limiting benign disease. The computed tomography (CT scan) lesion in these patients show a complete or near complete resolution on a subsequent scan while these patients are treated with antiepileptic drugs (AEDs) alone or along with other drugs.7 Since long there has been a lot of controversy regarding the treatment of patient of epilepsy with SSECT lesions. Many trials have been conducted in our hospital regarding treatment strategies in these patients. Initially, cysticidal drugs (albendazole or praziquantel) were used with AEDs in all patients of SSECT lesion with seizures, as recommended in other studies;8-11 however, later AED alone was found to be equally effective.12,13 There is, however, still a controversy regarding the duration of treatment with AED in these patients. Therefore, this study was planned in 81 patients of epilepsy with SSECT lesion in brain to determine the clinical profile and duration of antiepileptic drug treatment. Material and Methods Eighty one patients of SSECT lesion in brain with epilepsy were studied in Neurology department of G.B. Pant Hospital, New Delhi, from January 1996 to July 1999. All patients of epilepsy with small single enhancing CT scan/MRI brain lesion were included in the study. The diagnosis was based on CT findings of small (< 20 mm) single hypodense parenchymal brain lesion surrounded by edema and ring or disc enhancement in contrast CT scan. No patient had evidence of systemic illness including tuberculosis, neoplasia or acquired immunosuppression. These patients were randomly divided into two groups. Group A patients (41) were treated for 6 months and group B (40) for 1 year with antiepileptic drugs (AEDs). All patients were subjected to detailed history and physical examination for clinical profile and any associated disease. Complete hemogram, ESR, X-ray chest, Mantoux test, electroencephalography, CT scan or MRI brain were performed in all patients. Repeat imaging of brain (CT/MRI) was done at 3 months and/or 6 months after the first imaging, to see the changes in the SSECT lesion. All patients were followed up for one year after stopping AED. AED was continued for another 6 months in patients with persistent lesion on CT scan / MRI brain or in cases of recurrence of seizures. Patients with suspected tuberculoma or those treated with albendazole were excluded from the study. Results The commonest site of lesion was fronto-parietal in 36.5% in group A and in 45% in group B. The mean size of the lesion was 7.46±1.55 mm in group A and 7.55±1.79 mm in group B. Thirty six patients (87.81%) were seizure free in group A after six months of AED treatment and 35 (87.17%) in group B after one year of AED treatment. Recurrence of seizure occurred in 5 (12.19%) patients after 4.3±1.52 months of stopping treatment in group A and 5 (12.82%) patients after 2.2±1.48 months of stopping treatment in group B. Out of 5 cases of recurrence in each group, 4 (80%) had calcified lesion. Discussion Both groups A and B were comparable in terms of age and sex. In this study, high incidence of SSECT lesion was found in vegetarians, which has also been reported in earlier studies.13 Simple partial motor seizure with secondary generalization was the most common mode of presentation, which can be explained by focal parenchymal lesion present on CT scan/MRI brain. The most common site of the lesion was fronto-parietal corresponding to the type of seizure present in the study group. The mean duration of seizures was 2.5 months in group A and 3.9 months in group B. The mean number of seizure was 2.3 in group A and 2.5 in group B. The less number and duration of seizures showed the benign nature of disease which has also been shown in earlier studies.7,13,14 In a study conducted by Murthy and Subba Reddy,15 one episode of seizure was found in 63% cases and only 37% cases had recurrence of seizures, showing the benign nature of the disease. Large number of small single ring enhancing lesion on CT scan as compared to disc enhancing lesion probably showed the degenerating parasite. High percentage of disappearance of SSECT lesion at 6 months (63.41% in group A and 65% in group B) also showed the benign nature of the disease. In a study by Jain et al there was disappearance of lesion in 53% of cases at 6 months.16 Murthy and Subba Reddy15 reported disappearance of SSECT lesion in all the 102 cases on follow up CT scans. The disappearance of lesion was less at 3 months (group A-19.5%, group B- 17.5%) while it was higher at 6 months in both groups, suggesting that follow up CT scan should be done more appropriately at 6 months. The number of cases having persistence of lesion (4.87% in group A and 5% in group B) was also very less. Significantly high percentage of patients (group A 87.81%, group B 87.17%) had no recurrence of seizure after stopping the AED treatment in both groups. This indicates that short term AED treatment for 6 months is as effective as the one year therapy. Only five cases in each group had recurrence of seizures, and among these cases, 4 out of 5 patients (80%) in each group had calcified lesions. Jain et al reported 5% recurrence after stopping AEDs. It appears that the cause of recurrence is probably the calcified lesion. Garg and Nag14 reported that 9 out of 16 cases with persistent CT lesion had recurrence of seizure. Similar findings were confirmed by Murthy and Subba Reddy,15 while in our study the cause of recurrence was calcification. Conclusion This study reveals that SSECT lesion with epilepsy is a benign self-limiting disease. This randomized study has demonstrated that short term (6 months) AED treatment is as effective as one year treatment. The patients having calcified lesion, however, might require long term AED. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02042t1.jpg] [ni02042t2.jpg] |
| |||||||||

{kind=link}
{kind=link}