 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 153-157 Social Factors and Psychopathology in Epilepsy N. Cyriac, P.N. Sureshkumar, A.M. Kunhikoyamu, A.S. Girija* Departments
of Psychiatry and Neurology*,
Medical College,
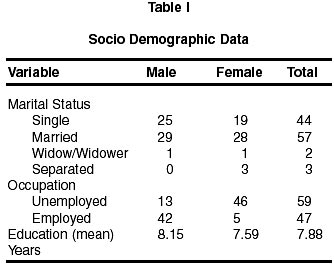
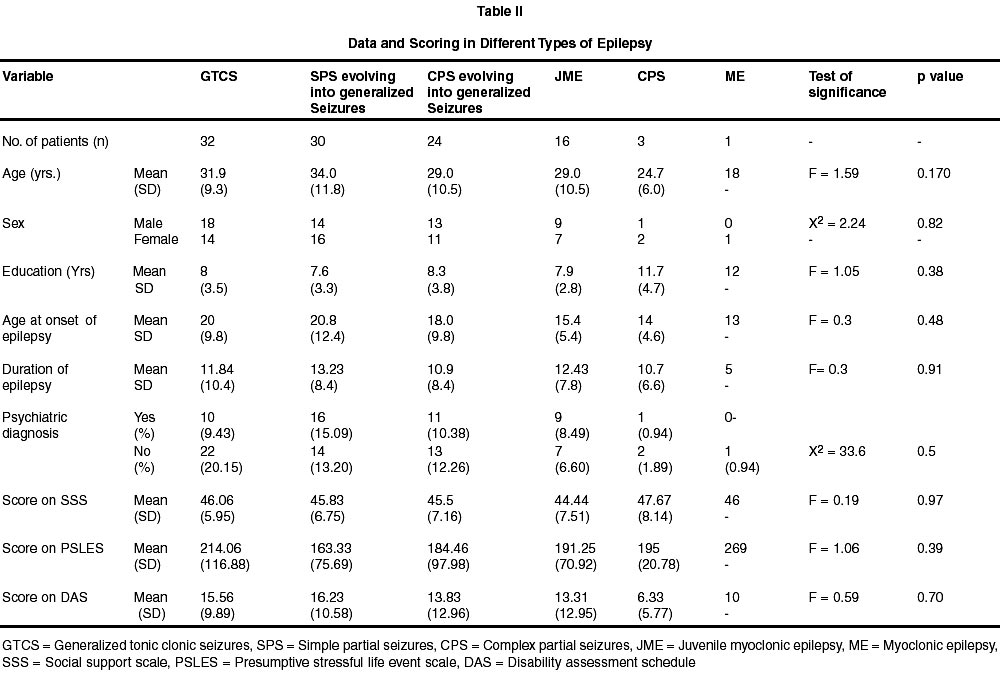
Calicut, Kerala, India. Accepted for publication : 20th March, 2001. Code Number: ni02044 Summary One hundred and six epilepsy patients were assessed over a period of 6 months for psychiatric morbidity, social support, stressful life events in previous year and disability. 45 patients (42.45%) had a psychiatric diagnosis. Organic depressive disorder headed the list (16.98%) followed by mild cognitive disorder (11.32%) and tobacco dependence (8.49%). There was no significant difference in the mean age, sex, mean education, age at onset of epilepsy, duration of epilepsy, psychiatric diagnosis, mean scores on social support scale, presumptive stressful life event scale and disability assessment schedule between different types of epilepsy. The difference in mean scores of presumptive stressful life events scale and disability assessment schedule between epileptics with and without psychiatric diagnosis was not statistically significant. Key words : Epilepsy, Depression, Cognitive disorder, Social support, Stressful life events. Introduction Epilepsy is a chronic neurological disorder associated with increased prevalence of psychopathology. The vulnerability factors and precipitating factors interact and cause decompensation of the precarious adjustment and result in psychiatric morbidity. Recent advances in the biological area have tried to find the organic basis of psychopathology in epilepsy.1-4 There has been lack of research into the role of psychosocial factors in predisposing the patients with epilepsy to a variety of psychopathology.5 The diagnosis of epilepsy is associated with social problems like stigma, discrimination in employment, difficulty in interpersonal relationships etc. For meaningful comprehensive management of patients with epilepsy, these aspect should also be dealt with. We conducted this study to assess the psychopathology, social support, life events and disability in patients with epilepsy. MATERIALS AND METHODS Study Design : This cross-sectional study was conducted in the Department of Neurology, Medical College, Calicut, over a period of 6 months from July 1999 to December 1999. Consecutive adult patients attending neurology clinic with epilepsy (diagnosed according to the ILAE Classification6 formed the study population. The patients who met ICD 10 research diagnostic criteria7 for mental retardation and patients unable to comprehend were excluded from the study. After obtaining informed consent, patients were assessed using: i) specially designed proforma for the study to assess socio-demographic data, details of epilepsy and anti-epileptic medication, ii) ICD-10 symptom checklist for mental disorders8 along with ICD 10 classification of mental and behavioural disorders - diagnostic criteria for research,7 iii) social support scale9 (SSS), iv) presumptive stressful life event scale10 (PSLES) and v) disability assessment schedule11 (DAS). Statistical Analysis : The results were tabulated with t-test, chi-square, analysis of variance (ANOVA), Pearson product moment correlation, Spearman correlation were used. Statistical package for social sciences (SPSS) was used for the above. Discussion One hundred and eleven patients with epilepsy were evaluated. Five patients were excluded. Three of them had organic mood disorder (two organic bipolar mood disorder and one organic manic disorder) and were unable to cooperate due to high distractability. Two patients had only pseudoseizures. Of the remaining 106 patients, 55(51.89%) were males and 51(48.11%) were females. The mean age of the sample was 30.96 (+10.44 years) with a range of 18-62 years. Majority of them were from rural area and were married. Three patients who were separated from their spouse were all females and stated epilepsy as the cause of their divorce. The mean education was upto 7.88 years. The socio-demographic details reflect the distribution in general population (Table I). Types of seizures seen in the group are mentioned in detail in Table II. Patients having different types of seizures did not vary significantly in mean age, sex distribution, mean education, age at onset of epilepsy, mean duration of epilepsy, psychiatric morbidity, social support, stressful life events in the previous year and disability (Table II). Out of 106 patients, 45 (42.45%) had psychiatric disorder. This is higher than the rates observed in earlier studies.12-14 This could be because the study was conducted in a tertiary care centre using semistructured diagnostic interview. Organic depressive disorder was the commonest psychiatric diagnosis (16.98%). This is at par with the general prevalence of 20-40%.14,15 Mild cognitive disorder constituted 11.32% followed by tobacco abuse/dependence. None of the patients were abusing alcohol or other psychoactive substances. Three patients had dissociative (conversion) disorder and two had emotionally labile (asthenic) disorder. One case with organic delusional (schizophrenia-like) disorder had CPS evolving to generalized seizures. Patients with psychosis usually do not attend neurology clinic and this could account for the very low prevalence (Table III) in this report. In this study, patients with SPS evolving into generalized seizures and JME had more psychiatric morbidity as compared to others (Table III). This is unlike earlier studies which showed significant association between psychomotor epilepsy (presently CPS) evolving into generalized seizures and psychiatric morbidity, especially psychosis.3,12,16,17 The difference between patients having psychiatric diagnosis and those who do not have, in the mean scores on stressful life events scale and disability assessment schedule between those with and without psychiatric disorders, was statistically significant (Table IV). The difference in mean score on social support scale was not statistically significant. Herman et al5 reported significant relationship between psychopathology and stressful life events in the previous year in epileptics. Low social support is linked to psychiatric morbidity, especially depression in general population.18,19 The results are in keeping with the current biopsychosocial model of psychiatric disorder, with the biological factors (anatomical or functional), precipitated by drugs or social factors, related to this4 References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02044t3.jpg] [ni02044t2.jpg] [ni02044t4.jpg] [ni02044t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}