 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 158-161 Correlation Between CT Scan and Automated Perimetry in Supratentorial Tumors S. Sood, N.K. Sharma,* M. Nada, A. Dutt, R.C. Nagpal Departments of Ophthalmology and Neurosurgery*,
Pt. B.D. Sharma Postgraduate Institute of Medical Sciences,
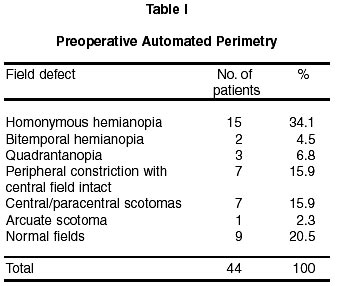
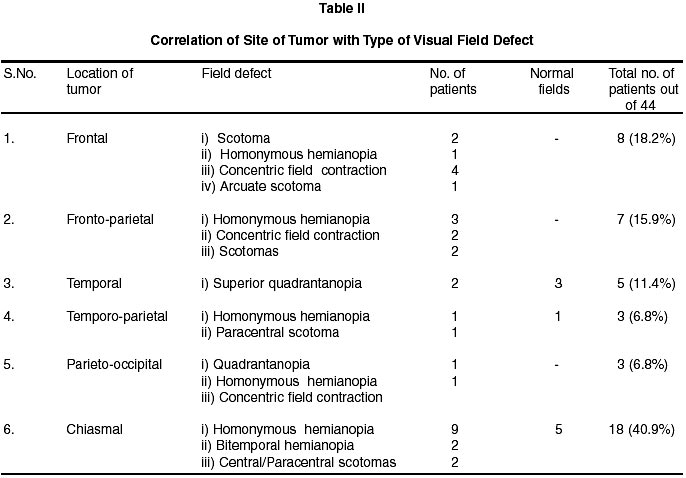
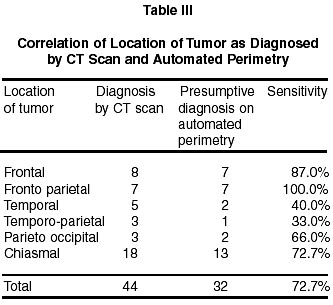
Rohtak - 124 001, India. Accepted for publication : 29th August, 2000. Code Number: ni02045 Summary An attempt was made to correlate various types of visual field defects on automated perimetry with the findings of computed tomography in 44 patients of supratentorial tumors. All the patients above the age of 10 years were subjected to complete neurological examination including investigations like plain X-rays and CT scan, however, MRI and angiography were performed wherever indicated. Ocular examination particularly pertaining to neuro-ophthalmological profile was carried out with special emphasis on automated perimetry on Humphrey field analyser. The results indicated that automated perimetry was capable of reliably detecting and quantitating the visual field defects and thus established the location of the tumor in 72% patients when compared to CT scan. Hence, any patient with neuro-ophthalmic features should be subjected to automated perimetry for early diagnosis and probable location of intracranial space occupying lesion affecting visual pathways. Key words : Supratentorial tumors, Automated perimetry, Homonymous hemianopia. Introduction Space occupying lesions or other intrinsic lesions of the brain are likely to manifest with ocular signs in the form of visual impairment, ocular motility disorder, papilledema and visual field defects. Among the ocular investigations, perhaps perimetry is of utmost importance.1-3 It points towards its probable topographical localization. Though there are a number of reports of intra cranial space occupying lesions (ICSOL) in relation to visual pathways with characteristic field defects, there are very few reports of distant supratentorial lesions producing field defects. In this study, various types of visual field defects were studied in patients of supratentorial tumors. A comparison between the topographical location of lesions as assessed by CT scan was made with that of automated perimetry. Material and Methods Fifty patients of intracranial space occupying lesions of supratentorial region, above 10 years of age, attending the neurosurgery OPD were included in the study, irrespective of the nature of pathology. However, patients with intracranial bleed from vascular lesions were excluded. All the patients were subjected to detailed general and neurological examination in addition to plain X-ray skull and CT scan. MRI and angiography were performed wherever indicated. The ocular examination included visual acuity, pupillary reactions to light and accommodation, alignment of eyes, ocular movements, intra ocular pressure (IOP) measurement, anterior segment evaluation, fundus examination, diplopia charting, perimetry (C-30-2 test primarily and FF-120 in patients who could not cooperate). CT scan was done in all the 50 patients, however, automated perimetry could be carried out in 44 patients only. Sensitivity test was applied in order to ascertain the sensitivity of automated perimetry as compared to the CT scan for locating the site of lesion. Results There were 31 (62%) male and 19 (38%) female patients. Maximum patients were found in age group range of 21-40 years (42%). Headache was the most common symptom (68%), followed by seizures (32%) and diminution of vision in 20% patients. 47(94%) right eyes and 44(88%) left eyes had maximal corrected visual acuity in the range of 6/6-6/12. Four patients had decreased vision to the extent of hand movements close to face to inaccurate perception of light. Seven patients with partial or complete optic atrophy had abnormal pupillary reactions ranging from sluggishness to complete absence of the reaction. Fundus showed optic atrophy in 8(16%) patients and papilledema in 4(8%) patients. Preoperative automated perimetry with Humphrey field analyzer using C-30-2 threshold programme in 44 patients showed homonymous hemianopia in majority of patients (34%) followed by central/paracentral scotomas and concentric field contraction in 15.9% patients each. Bitemporal hemianopia and quadrantopia were observed in 4.5% and 6.8% patients respectively. Normal fields were present in 20.5% of patients (Table I). Seven out of 9 patients of frontal lobe tumors had typical lesions like homonymous hemianopia, scotomas, concentric field contraction. In 7 of 8 patients of frontoparietal lesions, classical field defects were seen as shown in Table II. Classical field defect of superior quadrantanopia was seen in 2 patients of temporal lobe tumors. In chiasmal lesions, classical field defects of homonymous hemianopia and bitemporal hemianopia were seen in 9 and 2 patients respectively. Discussion The present study was designed in order to investigate neuro-ophthalmic patients and to correlate the findings with those of computerised tomography. In the present study of 44 supratentorial tumors, inclusive of 18 chiasmal tumors, all varieties of field defects were observed. The most common field defect observed was homonymous hemianopia in 34.1% of patients followed by peripheral constriction of fields and central and paracentral scotomas in 15.9% patients each. These findings were in accordance with another study where similar distribution of field defects was observed in 35% intracranial space occupying lesions.2 However, homonymous hemianopia was observed in 15% patients as compared to 34.1% patients in this study. This could be explained by the mismatching of patients samples in the two studies. In the present study, amongst chiasmal lesions, homonymous hemianopia was observed in 41% of the patients followed by bitemporal hemianopia and central/paracentral scotoma, which were observed in 9% each. This was in contrast to the observation of another study, where bitemporal hemianopia was seen in 69% patients.5 This appeared to be because of the fact that the type of patients included were purely pituitary related in their series as compared to sellar and parasellar lesions in the present study. The other reason could be that they had carried out the perimetry by tangent screen and Goldmann perimeter whereas it was carried out by Humphrey field analyser in the present study. Automated perimetry could be performed in 44 patients and the findings were correlated with that of CT scan (Table II). Field defects in 32 out of 44 patients were found to be very characteristic and typical, indicating the site of tumor, whereas the field defects in the other 12 patients were such that no conclusion could be drawn as regards to the location of the tumor. Out of these 12 patients, fields in 3 patients were non-specific and in 9 patients normal fields were observed. Non-specific lesions were observed in frontal lobe tumors. Normal fields were observed in 3 cases of pituitary tumors, 2 cases of craniopharyngioma, 2 cases of temporal glioblastoma, 1 case of tuberculoma and 1 case of temporoparietal lesion. Thus a good correlation between CT scan and automated perimetry as regards to the site of tumour could be drawn in the present study. The sensitivity of automated perimetry in diagnosing the site of tumor was 72.7% which was reasonably good. In another study, computer assisted interpretation of resolution of visual fields helped in the correct diagnosis of 64% of patients with chiasmal and 83% of patients with retrochiasmal tumors.6 The results in the present study were in conformity with that of Boglind6 since automated perimetry assisted in correctly diagnosing the location of supratentorial tumors in 72% patients. The foregoing discussion once again established that perimetry could be one of the most important tools in the complete investigation of a neuro-ophthalmic patients provided it is carried out by automated field analyzer. The results indicated that it was capable of reliably detecting and quantitating the visual field defects in patients of supratentorial tumors and thus assisted in establishing the diagnosis of location of the tumour in 72% of patients in the present series when compared with CT scan. Since the variable of perimetrist error can be automated, perimetry should always be preferred over kinetic manual and Goldmann perimetry in the evaluation of a neuroophthalmic patient. Therefore, any patient with neuroophthalmic features and unexplained deterioration of vision, with or without papilledema, should be subjected to automated perimetry for not only an early diagnosis, but even for the probable location of the intracranial space occupying lesion affecting the visual pathways. Automated perimetry thus provides a clue to the CT diagnosis in various supratentorial tumors. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02045t3.jpg] [ni02045t2.jpg] [ni02045t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}