 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Cardiovascular Responses to Scalp Infiltration with Reduced Concentration of Adrenaline B.K. Biswas, P.K. Bithal, H.H. Dash Department of Neuroanesthesiology,
All India Institute of Medical Sciences,
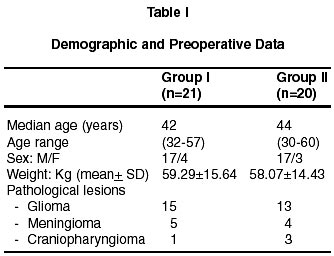
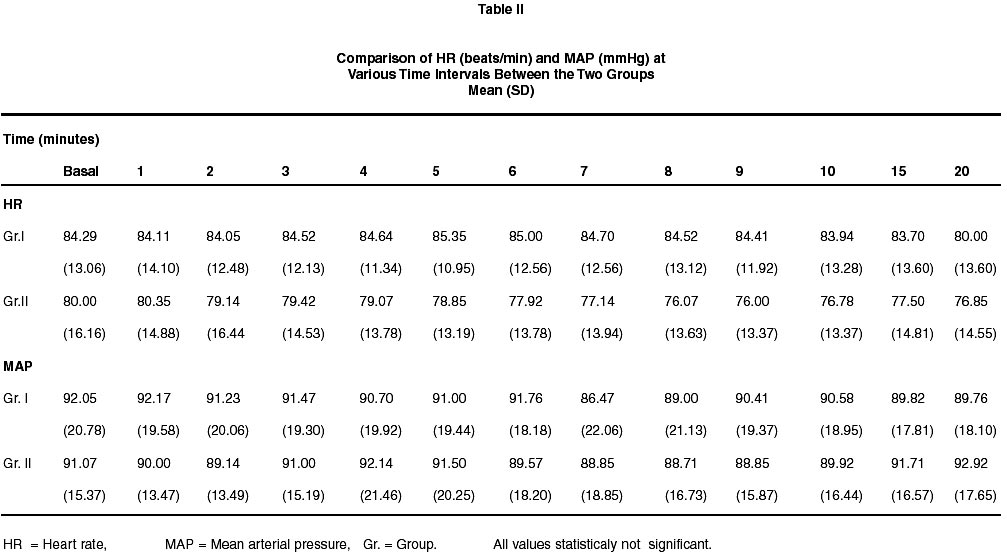
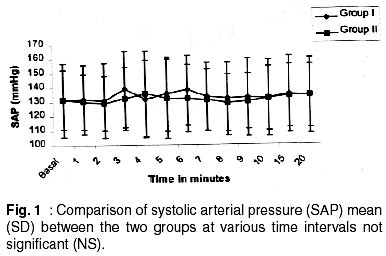
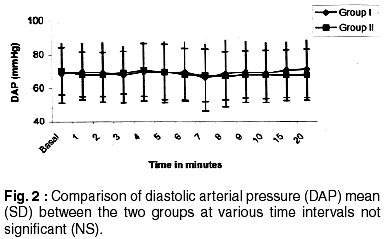
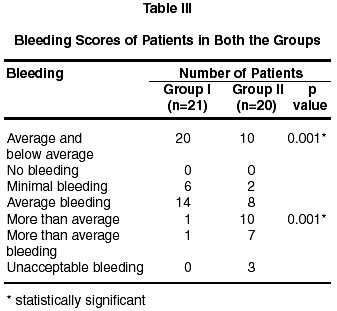
New Delhi - 110 029, India. Accepted for publication : 6th June, 2001. Code Number: ni02047 Summary A prospective randomized controlled study was carried out in 41 adult neurosurgical patients to find out the hemodynamic effects following scalp infiltration with 0.5% lignocaine with or without adrenaline. The patients were divided randomly into two groups. Group I patients (n=21) received 0.5% lignocaine with adrenaline (1:8,00,000) for scalp infiltration and group II patients (n=20) received 0.5% lignocaine without adrenaline. Continuous monitoring of ECG, heart rate and arterial blood pressure was carried out every minute for 20 minutes following scalp infiltration. Blood loss while raising the scalp flap was assessed by the neurosurgeon who was unaware of the study. No significant hemodynamic disturbances were observed in either group. However, Group I patients had significantly (p=0.001) less bleeding on incision. From this study, we conclude that 0.5% lignocaine with adrenaline (1:8,00,000) does not give rise to any cardiovascular disturbances during and following scalp infiltration. Rather, it minimises blood loss while raising the craniotomy flap. Key words : Neurosurgical anesthesia, Complications, Cardiovascular responses, Lignocaine, Adrenaline. Introduction Neurosurgical patients with space occupying lesions may have altered or inactivated autoregulation of cerebral blood flow (CBF). In such circumstances CBF is dependent on mean arterial pressure.1,2 Major hemodynamic changes such as alterations in blood pressure, heart rate and rhythm may have adverse effects like rupture of cerebral aneurysm and arteriovenous malformations or aggravation of ischemia in cases of subarachnoid hemorrhage with already existing vasospasm.3-5 Surgical stress resulting from scalp incision is one of the major causes of hemodynamic changes at the very beginning of surgery. For suppression of incisional stress and attainment of local hemostasis use of lignocaine (0.5%), with or without adrenaline, has been advocated depending upon the general condition of patients.6 Lignocaine with adrenaline in the strength or dilution of 1:2,00,000 is preferred, as it not only mitigates the incisional stress response but also minimizes bleeding during scalp incision.7,8 However, the major disadvantages of adrenaline (1:2,00,000) containing lignocaine infiltration is the hemodynamic disturbances that ensue following systemic absorption of adrenaline from a highly vascular area like scalp. Tachyarrhythmia, hypertension and even hypotension have been reported following the use of 0.5% lignocaine with adrenaline (1:2,00,000).8-10 In India however, due to non-availability of 0.5% lignocaine with 1:2,00,000 adrenaline we routinely use 0.5% lignocaine with 1:8,00,000 adrenaline for scalp infiltration prior to craniotomy. No study has been done to find out the efficacy of 0.5% lignocaine with adrenaline (1:8,00,000) in suppressing incisional stress response and also blood loss while raising craniotomy flap. To address the above issues, we carried out a prospective, randomized controlled study using 0.5% lignocaine with adrenaline (1:8,00,000) for scalp infiltration during craniotomies. Material and Methods Forty one adult neurosurgical patients between the age group of 21 and 65 years, of either sex, undergoing elective craniotomies were included in this study. The study was approved by the Hospital Ethics Committee and prior informed consent was obtained from all the patients. Patients with known cardiovascular disorders and diabetes mellitus were excluded from this study. They were randomly allocated into two groups. Group I patients received scalp infiltration with 0.5% lignocaine containing adrenaline (1:8,00,000) (10 cc of 2% lignocaine containing 1:2,00,000 adrenaline mixed with 30 cc of normal saline). Group II patients received 0.5% lignocaine without adrenaline for scalp infiltration. The surgeons were not aware of the nature of the solution used for scalp infiltration. All the patients were premedicated with oral diazepam 0.2mg/kg, 2 hours prior to anesthesia followed by a mixture of promethazine (0.5mg/kg) and atropine (0.05mg/kg) intramascular injection one hour prior to induction of anesthesia. Anesthesia was induced with thiopentone 4-5mg/kg. Suxamethonium 1.5mg/kg was used to facilitate orotracheal intubation. Anesthesia was maintained with 66% nitrous oxide in oxygen along with 0.4-0.6% isoflurane. Neuromuscular block was provided with pancuronium. Pethidine (1mg/kg) was used intravenously to provide intraoperative analgesia. All the patients were mechanically ventilated with the help of a ventimeter ventilator (Air Shield). The gas flow, tidal volume and respiratory rate were maintained so as to keep the end tidal carbon-dioxide tension around 30mmHg (Datex Capnomac). Continuous monitoring of electrocardiograph, heart rate, central venous pressure (by placing a central venous catheter through the arm vein) and intraarterial pressure (dorsalis pedis or posterior tibial artery) were carried out by a multichannel Mennen monitor (Horizon 1100). The pressure transducers were calibrated at the level of 5th intercostal space in mid axillary line. Data including heart rate, systolic blood pressure, diastolic blood pressure and mean blood pressure were stored in the monitor automatically at one minute intervals and were retrieved for analysis after the case was over. The total volume of infiltration used was 30 ml for all the patients. Intravascular volume status was maintained with crystalloid (Ringer's lactate and normal saline) infusion so as to maintain central venous pressure between 6-8 mm Hg. After scalp incision the surgeon was asked to assess the degree of bleeding as 1=nil, 2=minimal, 3=average, 4=more than average and 5= unacceptable. To make it more clinically relevant, the number of patients who had bleeding score of 1, 2 and 3 in each group were designated as 'average' or 'below average' category and likewise the patients who had bleeding score of 4 and 5 in each group were graded as 'above average category'. Statistical analysis was performed using multiple range test, Chi-square test and student's t- test. To compare mean and median values, student's t-test was used. Chi square test of proportions was applied to compare proportions. The p value of <0.05 was considered statistically significant. Results Demographic data and preoperative variables of all the 41 patients in two groups were comparable (Table I). Patients of neither group developed any significant changes in heart rate(HR), systolic blood pressure (SBP), diastolic blood pressure (DBP) and mean arterial pressure (MAP) (Table II, Fig. 1 and 2). However, in one patient of group I , at the end of two minutes following scalp infiltration there was more than 20% decrease in systolic, diastolic and mean arterial pressure, but it returned to normal at three minute. No significant differences in vital parameters were observed between the two groups of patients. Twenty patients of group I and 10 patients of group II had below average to average category of bleeding (p=0.001) (Table III). However, one patient of group I had blood loss which was graded as above average in comparison to 10 patients of group II (p=0.001) (Table III). Thus the patients in group I, who had average or below average category of bleeding, and the number of patients in group II, who had more than average category of bleeding, when compared with their counterparts of same category were statistically significant. This emphasizes that there was decreased amount of clinically relevant bleeding in patients of group I. No other intra-operative or post operative complication was encountered. Discussion Patients with intracranial pathology usually have impaired autoregulation of the cerebral circulation and CBF, instead of being flow dependent, becomes pressure dependent.1,2 During neurosurgical procedures it becomes desirable to suppress hemodynamic alterations for better cerebral protection. This can be achieved by infiltrating the scalp with local anesthetic before application of incision which obtunds the incisional stress response. However, a combination of local anesthetic with vasoconstrictor drug is preferred for infiltration, as it provides local hemostasis, thus minimizing blood loss and the need for blood transfusion.6 However, the dose of adrenaline for local infiltration is controversial. Different strengths of adrenaline have been used in different type of surgical procedures.9-12 In neurosurgical patients for cranial surgery no recommended dose of adrenaline is mentioned. The present study shows that scalp infiltration with lignocaine (0.5%) containing adrenaline in 1:8,00,000 strength does not give rise to any significant changes in heart rate, rhythm and arterial pressure. On the other hand, reduced concentration of adrenaline mimimizes surgical bleeding significantly at incision. Scalp is a highly vascular area and absorption of adrenaline should be rapid. Various studies have shown that the changes of vital parameters following infiltration of local anesthetic with adrenaline depend on physical status of the patient, amount of vasopressor used, vascularity of the site of administration and its rate of absorption from the area infiltrated.12-14 It has also been noted that the safe dose of adrenaline for infiltration can not be the same that is used for intravenously. However, a number of studies have pointed out that for infiltration in face, neck and head area, the safe dose of adrenaline mixed with lignocaine in the presence of isoflurane is 6 µg/kg. This dose of adrenaline becomes 3.4 µg/kg without lignocaine where lignocaine seems to be protective for heart.15,16 Such dose has been considered 'safe' because it did not produce any severe arrhythmia, paroxysymal ventricular contraction or severe hypertension. Fluctuation of hemodynamics even in normal range or moderately above the normal range have not been considered as detrimental in other studies involving other organ systems. But, such variations may be deleterious for patients with intracranial pathology who usually have deranged cerebral autoregulation. Thus, the recommended safe dose can not be accepted as safe for patients with intracranial pathology. In the study conducted by Muralidhar and Bhanumurthy the peak effect of hemodynamic alteration took place between 8-10 min after scalp infiltration of adrenaline (1:2,00,000) containing 0.5% lignocaine solution.7 However, we monitored the vitals for 20 min after scalp infiltration. Unlike their study, none of our patients developed tachycardia or hypertensive response after scalp infiltration. It can be assumed that less dose of adrenaline/kg body weight that has been used in our study may be the reason for this stable hemodynamics, because site of application are same in both the studies. The only difference was in the dose or strength of adrenaline used. Patients received 0.63 µg/kg (approx) adrenaline in our study while it was 5 µg/kg in their patients. If site of infiltration can be ignored, which in both studies was scalp, the marked difference must be on account of the dose of adrenaline that has been used in both the studies. The amount of adrenaline used in our study is thus acceptable for infiltration in scalp without the fear of hemodynamic disturbances. One of the patients in adrenaline group developed hypotension in the present study. It is very difficult to correlate this fact with myocardial depression by anesthetics, hypovolemia or vagal response to stretching of galea which seems unlikely as the anesthesia technique and intravenous fluid therapy remained constant in all the patients. Phillips et al endorsed the hypothesis of b2 receptor stimulation by low dose of adrenaline causing skeletal muscle vasodilatation and documented hypotension (> 20% fall) in 47.5% of patients following scalp infiltration with adrenaline (1:2,00,000) containing local anaesthetic.10 Adrenaline in the dose of 0.1 µg/kg causes the arterial pressure to decrease because of its greater effect on skeletal b2 vascular vasodilator receptors than a1 vasoconstrictor receptors.10,17 Is this hypotension observed in our study due to its effect on b2 receptors ? It can be presumed that the patient might have developed such concentration (0.1 µg/kg) either due to more rapid absorption from scalp site or may be due to deranged pharmacokinetics of adrenaline. A more sensitive b2 receptor than other patients may also be the another reason for development of hypotension. This needs further study. Our study was not a double-blinded one and to overcome this error we stored the data automatically in the cardiac monitor during the study period. The most intriguing observation was the surgeon's grading of scalp bleeding during elevation of skin flap. Despite reduced concentration of adrenaline there was effective control of bleeding during skin incision. Besides statistical significance, minimal blood loss was observed not only by one surgeon but also by several others who were not aware of the nature of the solution. Therefore, it can be presumed that even lesser strength of adrenaline gives adequate concentration at the site of infiltration producing enough local vasoconstriction and excellent local hemostasis. We recommend routine use of 0.5% lignocaine with reduced concentration of adrenaline (1 in 8,00,000) as it provides the following benefits: (i) it helps in obtundation of surgical stress, thereby minimizing cardiovascular response, (ii) blood loss is meagre and it provides relatively dry field for surgical procedures, (iii) if needed, larger volume can be infiltrated as adrenaline in such reduced strength produces least hemodynamic alterations. Further clinical research is needed to find out its usefulness in patients with cardiovascular diseases and diabetes mellitus. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02047t3.jpg] [ni02047t2.jpg] [ni02047t1.jpg] [ni02047f1.jpg] [ni02047f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}