 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 184-186 Valley Sign in Duchenne Muscular Dystrophy : Importance in Patients with Inconspicuous Calves S. Pradhan Department of Neurology,
Sanjay Gandhi Postgraduate Institute of Medical Sciences,
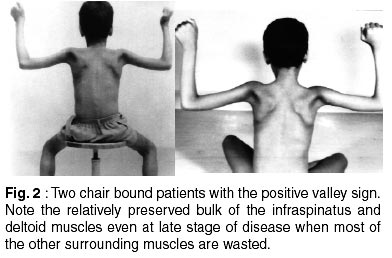
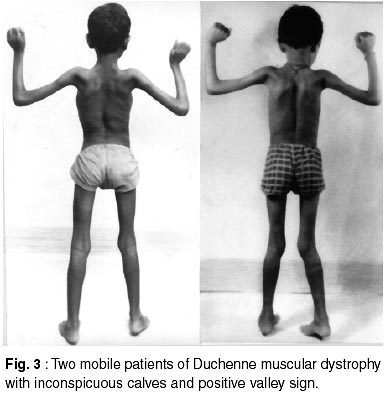
Lucknow - 226 014, India. Accepted for publication: 28th August, 2001. Code Number: ni02050 Summary Several patients of Duchenne muscular dystrophy (DMD) do not demonstrate clinically remarkable calf hypertrophy. A new clinical sign visible behind the shoulders, which may be called 'valley sign', was tested for its utility in such cases as clinical diagnosis becomes difficult in these patients. Out of 142 DMD patients seen in the last 7 years, 12 were found to have inconspicuous calves. All the 12 patients had clinical, biochemical and/or genetic evidence of DMD. The new sign was examined by 3 independent observers in these 12 DMD patients and in 10 patients with other neuromuscular diseases. Eight DMD patients and none of the others showed positive sign. This signifies importance of this sign in the clinical diagnosis of DMD in those children in whom the calf muscle bulk is apparently normal. Key words : DMD, Valley sign, Dystrophin gene, Muscular dystrophy. Introduction Selective muscle involvement is an important characteristic of muscular dystrophies.1 In Duchenne muscular dystrophy (DMD), this selectivity is evident for hypertrophy as well as wasting.2 The clinical observations on muscle bulk in DMD suggest infraspinatus and deltoid to be the second and third most common hypertrophied muscles after the calf. The anterior and posterior axillary folds are the most significantly wasted muscles.3 Still finer observations have revealed that in deltoid muscle, only the central fibres originating from the acromion process are enlarged while anterior and posterior fibres originating from clavicle and spinous process of scapula respectively, are wasted.3 Similarly, the inferomedial part of infraspinatus muscle is enlarged while the superolateral part is wasted. In other words, even though deltoid and infraspinatus muscles are enlarged, parts of these muscles along with the other muscles, which traverse through the posterior axillary fold, are wasted.3 On the other hand, subtle enlargement of a muscle is best observed when the muscle in question is under mild contraction.3 Based on these findings, a new clinical sign has been described.4 The sign which may be called 'valley sign' has specificity for DMD with sensitivity of about 90%. In the present clinical study, this sign was tested in those DMD patients who had no calf enlargement on first examination. Material and Methods Out of 142 patients of DMD seen in outpatient clinic in previous 7 years, 12 were found to have normal bulk or inconspicuous enlargement of the calf muscles during their first clinical examination. These 12 patients were selected for the present study. The criteria to call these patients as having DMD included typical history and physical findings of DMD, clinical evidence of gradual progression of the disease, medical records showing markedly raised serum creatine phosphokinase levels at some stage during the course of disease and myopathic pattern on concentric needle electromyography. Family history of typical progression of disease from onset to chairbound stage, typical histopathological findings in patients or affected siblings and deletion of the dystrophin gene, were taken as the definitive evidences whenever present. Gene deletion studies were performed in all patients by the method described in earlier reports.3-5 Sign detection To view the sign, the back of the child was exposed. He was asked to abduct the shoulders to 90° or thereabout, with 90° flexion of the elbows, so that the hands were directed upwards (Fig. 1). In patients with DMD, two bulges were visible on either side of a depression on the back of the shoulder, like a valley between two mounts.4 The depression or groove ran from the spinous process of the scapula to the axilla, and was due to wasting of the muscles in the posterior axillary fold. Inferomedial to this depression was the bulge (the mount) due to hypertrophy or the relatively preserved bulk of the infraspinatus muscle; superolateral to the depression was the bulge (the second mount) due to hypertrophy or the relatively preserved bulk of the deltoid muscle (Fig. 1). All the 12 patients selected for the present study were examined for this clinical sign. The sign was evaluated by the author and final decision regarding its positivity was taken after gathering independent opinions of two postgraduate doctors getting training in Neurology. Ten patients in the age group of 6-13 years who were suffering from neuromuscular diseases other than DMD, were also studied for this sign. These included 4 patients with limb girdle muscular dystrophy, 4 patients with spinal muscular atrophy type III, one patient with renal osteodystrophy and one patient with facio-scapulo-humeral muscular dystrophy. Diagnosis of these patients was supported by clinical, biochemical, electrophysiological and/or histopathological evidences. The sign observed in DMD patients was compared with the findings seen in these patients. Results Out of 12 patients, 9 were chair-bound at the time of examination. All the chair-bound patients (aged 12-15 years) had onset of symptoms (as noted by their parents) at 3-4 years of age and progression to chairbound stage at 11-12 years of age. All had medical records showing enlarged calf muscles, positive Gower's sign and very high serum CPK values ranging from 5,200 IU to 18,600 IU during the earlier course of their disease. The bulk of the calf muscle however, had resolved to normal after their attainment of chair-bound stage. During clinical examination at this centre, their serum CPK values ranged from 1800 IU to 5600 IU. Five of them were positive for deletion of the dystrophin gene. Of the other 3 mobile patients, one (7 years old) had serum CPK value of 12500 IU (with his 2 affected relatives having enlarged calves) and the other 2 (aged 8 and 9 years) had very high serum CPK values (10400 IU, 8600 IU) and positive gene deletion studies. The sign was positive in 6 chair bound (Fig. 2) and 2 mobile patients (Fig. 3). All the 3 chair bound patients with negative sign had significant wasting of posterior axillary folds. However, one of them had marked obesity that masked the sign. The other two had absence of infraspinatus and deltoid hypertrophy probably by the same process that resolved the calf hypertrophy. The only mobile patient with negative sign was a 7 years old boy whose infraspinatus and deltoid muscles showed minimal enlargement but the wasting of the posterior axillary fold was not significant enough to produce a depression between the two bulges. Conversely, the 6 chair bound patients with positive sign had relatively preserved bulk of infraspinatus and deltoid muscles and the sign was visible mainly due to marked wasting of the posterior axillary folds (Fig. 2). Patients other than DMD did not show this sign even though infraspinatus hypertrophy was observed in two patients with SMA. Discussion The present study demonstrates the validity of valley sign in those DMD patients who do not have prominent calves. The sign is based on an essential phenomenon of selective muscle involvement in muscular dystrophy which, in the case of DMD, is present for hypertrophy as well as wasting.3 Interestingly, the selectivity is so marked that both hypertrophy and wasting could be observed in the same region i.e., on the back of the shoulder.4 The present study deals with only those 12 DMD patients who were found on first clinical examination to have absence of prominent calves. Presence of a positive sign even when the calves had failed to enlarge in early stages of the disease or had resolved to normal bulk during late stage, indicates that the regional topography of muscles behind the shoulder remains maintained in early as well as late stages of the disease and that this is perhaps more consistent finding than the calf hypertrophy itself. A recent review has compared this new clinical sign with the Gower's sign.6 The Gower's sign is based on selectivity in the loss of muscle power in certain groups of muscles so that the child makes best use of relatively preserved muscle power (in spared groups of muscles) which can be appreciated in the peculiar way the child gets up from squatting position. Thus, one can infer that the Gower's sign highlights selectivity in the loss of muscle power, while this new clinical sign highlights selectivity in the loss of (or the increase in) muscle bulk.6 The valley sign, apart from its routine use, may have a clinical value in those DMD patients who have inconspicuous calves. Acknowledgement The author gratefully acknowledges the help of Dr. B. Mittal, Department of Genetics for performing gene deletion studies and Dr N. Pandey, and Dr. A. Kumar, who helped in the clinical assessment of the patients. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02050f2.jpg] [ni02050f1.jpg] [ni02050f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}