 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
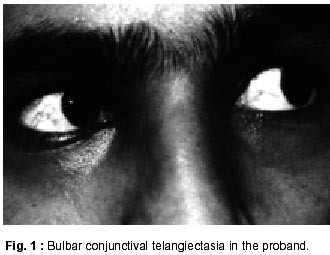
Neurology India, Vol. 50, No. 2, June, 2002, pp. 187-189 Dystonia as Presenting Manifestation of Ataxia Telangiectasia : A Case Report V. Goyal, M. Behari Department of Neurology,
All India Institute of Medical Sciences,
New Delhi - 110 029, India. Accepted for publication : 6th June, 2001. Code Number: ni02051 Summary Ataxia telangiectasia is a genetically inherited multisystem disorder with predominant feature being telangiectasia and cerebellar ataxia. In this report, a family of three siblings suffering from ataxia telangiectasia is described. The proband presented with dystonia and dystonic myoclonus, both of which are rare presenting features of ataxia telangiectasia. Key words : Ataxia, Telangiectasia, Dystonia, Myoclonus. Introduction Ataxia telangiectasia (AT) is a genetically determined autosomal recessive, multisystem disorder causing neuro-degeration and immunological abnormalities resulting in increased susceptibility to infection and malignancies, endocrine deficiencies, increased sensitivity to ionizing radiation and an anomaly of DNA repair. The ataxia manifests as the child starts walking while ocular telangiectasia is usually appreciated around 4-6 years of age. Vessels over exposed bulbar conjunctiva become prominent and appear fan shaped. Neurological manifestations consist of ataxia, choreoathetosis, ocular movement abnormalities, mental retardation and dystonias. Syllaba and Henner first descirbed this condition in 1929.1 We report a patient of AT who presented with generalized dystonia. Case Report A 13 year, right handed girl, second of the three siblings, product of non-consanguineous marriage with normal birth and early milestones, presented with turning of neck and twisting of trunk towards right side for the last 6 months. Six weeks after onset of symptoms, she developed abnormal posturing of right upper limb causing adduction of arm and pronation of forearm. Soon, her right foot was also involved causing plantar flexion and inversion. These dystonic movements were initially present only during action and progressed in 2-3 months time, to be present at rest as well. Within a month, she developed slurring of speech and sudden jerking movements of upper limbs and trunk. She had primary amenorrhoea. Her scholastic performance had been deteriorating for the past 4-5 years. She used to have recurrent respiratory tract infections, particularly during winter months. General physical examination showed bilateral conjunctival telangiectasia (Fig. 1). Her secondary sexual characters were pooly developed. She was mentally subnormal. She had ocular apraxia, cervical dystonia resulting in retrocollis and laterocollis. There were asymmetrical (right more than left) choreoathetotic movements involving both upper and lower limbs with dystonic posturing of trunk (correctable kyphoscoliosis), which deteriorated markedly during walking. Along with this, she had myoclonic jerks involving the upper limbs and trunk. She also had bilateral cerebellar signs (right more than left) with dysarthric speech. Fundi and retinal examination was normal. Joint and position sensations were bilaterally impaired in lower limbs distally. Bilateral ankle reflexes were sluggish with flexor plantar response. Slit lamp examination for Kayer- Fleischer ring was negative. Laboratory investigations revealed normal hemogram, serum calcium, phosphorus and electrocardiogram. Serum alfafetoprotein (AFP) was raised (147 IU/ml, normal = < 30 IU/ml), serum IgG (1060 mg/ml, normal = 800- 1700 mg/ml) and IgA (188 mg/ml, normal = 85-450 mg/ml) levels were within normal limits. MRI of brain showed mild cerebellar atrophy bilaterally (Fig. 2). Motor nerve conduction studies were normal. Sensory nerve conduction study revealed that action potentials were not recordable from sural nerves. She had moderate improvement in her truncal dystonia with trihexyphenidyl. Her 15 year old elder brother and 8 year old younger brother had classical cerebellar ataxia and telangiectasia. Both had mental retardation and sensory neuropathy. Discussion Common presentations of AT include cerebellar ataxia, ocular telangiectasia, immunodeficiency and movement disorders. Choreoathetosis is the commonest extrapyramidal feature present in 90% of cases.2,3 In India, AT was first reported by Dogra and Manchanda.4 Various atypical presentations of AT have been described. Dystonia usually develops as a late manifestation and has been reported in 71% of patients.3 Dystonia as a presenting feature is very rare. Dystonia has been rarely described in adolescents and adult patients too.5,6 The index case presented with dystonia even before development of cerebellar symptoms, which is very rare. Another unusual feature in this case was dystonic myoclonus involving upper limbs and trunk. Myoclonus has been described in 16 of 70 patients in a series by Woods and Taylor, of which 7 patients also had episodic distressing and involuntary shaking of one limb.3 In later stages of AT, it may be difficult to differentiate AT from Friedreich's ataxia (FA) in presence of neuropathy. Presence of telangiectasia, absence of posterior column dysfunction and elevated AFP usually help to differentiate one from the other. Electro-oculogram (EOG) finding can also differentiate AT from FA.7 EOG shows normal saccadic velocity but abnormal initiation of saccade in AT.7 In our case, AFP was raised and immunoglobin levels were within normal range. In an Indian series of 22 patients, IgG was normal in all patients but IgM was low in 2 of 18 patients tested.8 Secretary IgA was absent in all the 18 patients. MRI brain of index case showed only mild cerebellar atrophy. Nerve conduction study showed sensory neuropathy in the patient and her siblings. According to reports, the nerve conduction velocities are normal in young patients whereas older patients show predominantly sensory neuropathy, as in our case.6,9 Bodensteiner et al10 reported a 10 year old boy, who presented with neck, trunk and upper limb dystonia which progressed over months, masking his cerebellar signs. Treatment with haloperidol improved the dystonia partially with worsening of his cerebellar signs. Though myoclonous has not been described in literature but jerks involving whole limbs and episodic distressing involuntary shaking of one limb were reported by Woods and Taylor, in few of their patients.3 All the alive siblings of the patient with dystonia should be examined for telangiectasia. As these patients are abnormally sensitive to ionizing radiation, radiological investigations should be planned carefully. They should be evaluated frequently, once in 6-12 months, for early diagnosis of malignancies, especially lymphoreticular malignancies. The risk of developing leukemia and lymphomas is 70 and 250 times of normal population, respectively.11 Lymphoreticular neoplasm and leukemias are more common in pre-adolescent patients, whereas epithelial tumors occur more commonly in post adolescent age group.9 Heterozygous and blood relatives also have excess risk of malignancies, particularly breast cancer in females. Cells derived from homozygous and heterozygous persons are unusually sensitive to ionizing radiation. Therefore, these patients require special care to reduce industrial and unnecessary diagnostic exposure to ionizing radiation to prevent these malignancies. As histopathological finding is rarely reported in literature, exact neuropathogenesis of various symptoms is not clear. Neuropathologically prominent or ectatic blood vessel or frank vascular malformation are occasionally seen in brain.4,12 Multifocal areas of reactive astrocytic gliosis are found in brain.5 Though histopathologically vascular abnormalities have been reported, Hassler failed to demonstrate telangiectasia in cerebral parenchyma by microangiography.13 The exact pathogenesis of dystonia in AT is unclear, it could be due to vascular abnormality in basal ganglia or secondary changes in basal ganglia due to altered hemodynamics resulting from vascular abnormality in nearby parenchyma. This hypothesis needs to be tested. This patient of AT presented with dystonia. She also had myoclonic jerks (dystonic myoclonus), which is an unusual movement disorders in AT. This family is also unusual in that the youngest sibling had electrophysiological evidence of peripheral neuropathy when examined at the age of 8 years. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02051f2.jpg] [ni02051f1.jpg] |
| |||||||||

{kind=link}
{kind=link}