 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 194-197 Schizencephaly Associated with Bipolar Affective Disorder P. Relan, S.K. Chaturvedi, B. Shetty* Departments of Psychiatry,
National Institute of Mental Health and Neurosciences
and
Chief Radiologist*
Medinova Labs,
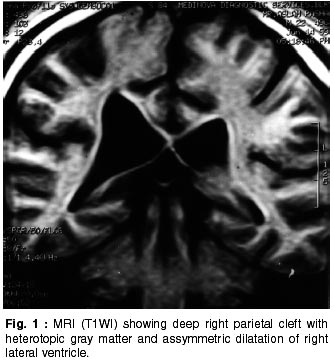
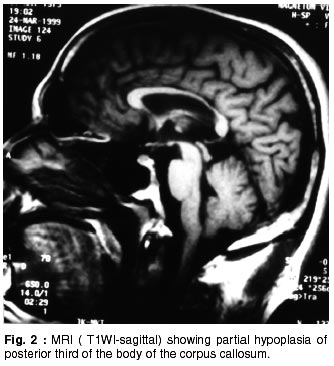
Bangalore - 560 029, India. Accepted for publication : 12th May, 2001. Code Number: ni02053 Summary Schizencephaly is a rare congenital anomaly of the brain, characterized by formation of abnormal unilateral or bilateral clefts in the cerebral hemispheres. It often manifests with partial seizures, mental retardation and hemiparesis. Only two cases of schizencephaly associated with psychosis have been reported in the literature. A patient of schizencephaly, who had bipolar affective disorder is described. It has been compared with the earlier two reported cases of schizencephaly associated with pyschosis. Key words : Schizencephaly, Bipolar affective disorder, Neurodevelopmental anomalies. Introduction Schizencephaly, originally described by Wilmarth and later named so by Yakolev and Wadsworth, is a rare congenital disorder of cerebral cortical development.1-3 It is a neuronal migration anomaly, caused by insults to migrating neuroblasts during 3rd to 5th gestational months. Other anomalies in this category include agyria, pachygyria, polymicrogyria, unilateral megalencephaly, gray matter heterotopias, lissencephaly and agenesis of corpus callosum.4,5 Basically, schizencephaly is characterized by a cleft traversing cerebral hemisphere, infolding of cortical gray matter along the cleft, an abnormal ventricular system and other associated cerebral anomalies.6 The MRI scan depicts the above findings. A key feature on MRI is the presence of ventricular dimple, which is almost always seen in cases with closed lip schizencephaly. Mild hypoplasia of corpus callosum along with septo- optic dysplasia is very common.7 It could be unilateral or bilateral, depending on the cerebral hemispheres involved. Schizencephalic cleft occurs more often in the anterior than in posterior neocortex.3 Clefts most commonly involve the parasylvian region and have been divided in two subtypes. Type I have fused lips and Type II have separated lips. Thus, there are four categories defined radiologically i.e. unilateral open lip (36.2%), unilateral closed lip (25.6%), bilateral open lip (25.6%) and bilateral closed lip (12.8%). 3 Schizencephaly may occur due to various causes. It may be due to localized ischemia in periventricular germinal matrix,8 or it may be an extreme variant of cortical dysplasia, in which the infolding of cortex extends all the way into the lateral ventricle.9 A report of schizencephaly in two affected sibs suggested genetic basis10 and indicated the possibility of autosomal recessive form of transmission.11,12 Schizencephaly has recently been associated with a germline mutation in homeobox gene EMX2 in 70% of patients.12 CMV infection, postnatally, has also been blamed in its complex multifactorial pathogenesis.13 Intoxicants, radiation2 and intrauterine exposure to warfarin have also been associated with this anomaly.14 Age at detection ranges from 8 months to 30 years. Clinical manifestations vary from mild to severe and include developmental delay and retardation, microcephaly, language dysfunction, focal or generalized motor abnormalities and seizures.6 Closed lip schizencephaly usually presents with hemiparesis or motor delay, whereas patients with open lip schizencephaly present with hydrocephalus. Neurodevelopmental outcome is generally poor with 51% showing severe deficits and 32% moderate impairment. However, 17% have mild or no problem. Closed lip schizencephaly is more likely to be associated with better outcome than open lip schizencephaly (78% versus 31%). Language development is significantly more likely to be normal in patients with unilateral schizencephaly as compared to those with bilateral clefts (48% versus 6%). Thus, presentation and outcome vary but are related to the extent of cortical involvement.3 Psychotic symptoms have been reported in association with a wide array of brain abnormalities or injuries, but there is just a single published report on psychotic symptoms in two patients with schizencephaly. In this case, another patient with schizencephaly who had bipolar affective disorder (mania with psychotic symptoms) with mild mental retardation reported and it is compared with the two cases reported earlier.1 Case Report A, 20 years male, from middle socio-economic strata, working irregularly as a furniture polisher, was brought with complaints of overactivity and overtalkativeness to the psychiatry out patient clinic at the National Institute of Mental Health and Neuro Sciences, Bangalore, India. Patient has a cousin (paternal uncle's daughter) aged 11 years, who is a dwarf (almost 2 feet). Patient was well adjusted premorbidly. He was 4th of 6 sibs, born as a twin along with a sister, in a hospital as full term vaginal delivery, had postnatal hyperbilirubinemia, for which he was given phototherapy for about a month and had birth weight of about 1.4 kilograms. There was no history suggestive of intrauterine exposure to any drug or radiation or any postnatal viral infections. He achieved milestones at fairly normal timings. Since the age of 4 years he was found to have weakness of left upper and lower limbs. Learning difficulties became obvious in the 2nd year of schooling at the age of about 7 years, so the family removed him from school. At the age of 10 years he had an episode of mania characterized by disturbed sleep and appetite, being overtalkative, overactive, oversocial, overreligious, cheerful, with occasional irritability for about 6 months. He reported delusions of grandiosity (identity and ability), occasional persecutory ideation and II and III person auditory hallucinations of commanding type. He was totally asymptomatic till about 3 years back when he started having similar episodes lasting 3 months and occurring every 2 months, but reached premorbid levels in between. Present episode had been prolonged for more than 4 months and was continuing even at the time of consultation. He had been on various antipsychotics without much improvement. General physical examination showed left arm fixed in midprone position and patient was unable to perform pronation-supination movements. Radiography did not show any bony abnormality. Left lower limb was about 1 inch shorter than the right and he walked with a limp. Oral examination showed high arched palate. Intelligence test showed IQ of 54 units i.e. mild mental retardation, as per ICD-10.15 Neuropsychological assessment revealed poor processing in neuro-cognitive psychological motor areas tested. There was no evidence of scatter or lateralization of deficits. Results of all blood tests (hemogram blood sugar and electrolytes, liver function tests, kidney function tests, RA and ANA factors), chest radiography, ECG and EEG were within normal limits. CT scan and MRI scan showed asymmetric dilatation of right lateral ventricle. A dimple was observed in the right lateral ependymal surface. MRI scan also revealed deep right parietal cleft with heterotopic gray matter along with partial hypoplasia of posterior third of body of corpus callosum. Septum and optic nerves were normal (Fig. 1 and 2). Thus, radiological findings confirmed right closed lip schizencephaly with partial hypoplasia of corpus callosum. The twin sister's CT scan was reported to be within normal limits and she was clinically found to be maintaining well. The patient was treated with Loxapine liquid (5-7mg hs). Later on, in view of the affective disorder, he was prescribed carbamazepine 800 mg per day for prophylaxis. He showed good improvement in 3 weeks and was maintaining near total improvement at the time of discharge and had reached premorbid levels of functioning. Follow-ups at 3 weeks, 6 weeks and 6 months showed patient to be euthymic and without any psychotic symptoms or behavioural abnormalities. Discussion The present case has clinical manifestation of schizencephaly, like mental retardation and mild motor impairment, besides the radiological evidence. However, this case did not have microcephaly, language dysfunction or seizure. Alexander et al discussed the importance of association between schizencephaly and psychosis.1 The present case, demonstrates an association between schizencephaly and bipolar affective disorder. A similar association was noticed by Black and Kilzieh.16 They found schizencephaly on investigation in a patient of psychotic bipolar depression after the patient developed multiple movement disorders after getting imipramine. On comparing the present patient with the earlier two reported patients there are some similarities between them.1 He had closed lip schizencephaly like one of the patients, but was unilateral. Both the cases had mental retardation and both showed moderate to good response to treatment, which seems to keep in line with the notion that closed lip schizencephaly is more likely to be associated with better outcome.3 The patient reported earlier had other problems like delayed milestones, seizures, depressive symptoms, suicidal ideas and the eye problems, which the present patient did not have. On comparing with the other reported patient, who has unilateral schizencephalic cleft, we note that both these patients had the postnatal hyperbilirubinemia. The second patient had family history of mental illness which none of the other two had. He did not have mental retardation, however, his response to treatment was poor. All the three patients have had some motor impairment and had psychotic features characterized by auditory hallucination and delusions. The comparison does not confirm any definite trend of common features in cases of schizencephaly with psychosis. The possible association between the bipolar affective disorder and schizencephaly in the present patient indicate the role of neurodevelopmental abnormality in the manifestation of bipolar affective disorder of early onset. But we wonder whether it is just a chance association. Nevertheless, presence of neurodevelopmental anomalies may have pathoplastic effects on the presentation of psychosis and may also influence treatment response adversely, as in the earlier cases. More similar reports could throw more light on neuro developmental deficits in psychosis. Whenever clinicians suspect such abnormalities they should do a thorough radiological investigation for confirmation. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02053f1.jpg] [ni02053f2.jpg] |
| |||||||||

{kind=link}
{kind=link}