 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 2, June, 2002, pp. 198-200 Infrasellar Craniopharyngioma Mimicking a Clival Chordoma : A Case Report R. Kachhara, S. Nair, A.K. Gupta,* V.V. Radhakrishnan,** R.N. Bhattacharya Departments of Neurosurgery, Radiology* and Pathology**,
Sree Chitra Tirunal Institute of Medical Sciences and Technology
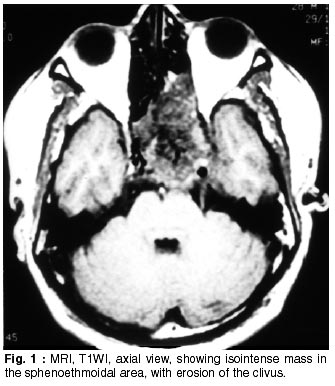
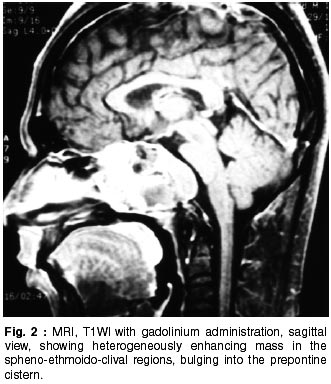
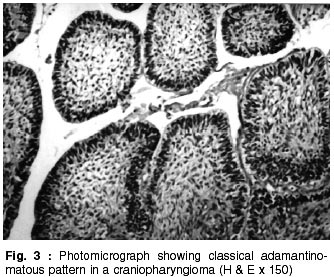
Trivandrum-695 011, India. Accepted for publication : 6th February, 2001 Code Number: ni02054 Summary An unusual case of entirely infrasellar craniopharyngioma mimicking a clival chordoma is described. Only 22 cases of craniopharyngioma with nasopharyngeal extension have been reported in the literature. Of the reported cases, most were primarily intracranial with secondary downward extension; only two were thought to originate from an infrasellar location. The present case is another example of an entirely infrasellar craniopharyngioma, with extensive clival destruction, mimicking a clival chordoma. Relevant literature on the subject is reviewed. Key words : Craniopharyngioma, Chordoma, Nasopharyngeal neoplasms. Introduction Craniopharyngiomas are benign neoplasms arising along the path of the craniopharyngeal duct and most frequently located in the sellar or suprasellar region. Uncommonly, they extend to the anterior, middle and posterior cranial fossa or to the infrasellar area. A case of giant craniopharyngioma originating entirely in the infrasellar region i.e. sphenoid sinus, ethmoid sinus and nasopharynx and causing gross destruction of the clivus, thus mimicking clival chordoma, is described. Only 22 cases have been reported in the available literature.1-18 Of the reported cases, most were intracranial with secondary downward extension; only two were thought to originate from an infrasellar location.19,20 We describe another similar case which was near totally excised through an extended transbasal approach. Case Report A 28 year old man, painter by profession, was admitted under neurosurgery with the chief complaint of headache for 8 months. Headache was mainly bifrontal, mild to moderate severity, dull aching in character, without any diurnal variation and unassociated with vomiting. It used to get relieved by analgesics. Eight weeks prior to admission, he also noticed blurring of vision for distant objects and occasional diplopia in the left eye. General physical examination was normal except for short stature and right scrotal hydrocele. He had well developed secondary sexual characters. Neurologically, he was conscious, alert and oriented. Visual acuity, visual fields and fundi were normal. He had minimal left abducens paresis. Rest of the neurological examination was within normal limits. His biochemical and hematological parameters were found to be normal. A plain X-ray skull, lateral view, showed gross destruction of the sella and clivus, with dense calcification in the sellar region. CT without contrast administration, revealed an iso- to hyperdense mass in the sella, sphenoid sinus, ethmoid sinus and the nasopharynx with areas of dense calcification in sella and destruction of the clivus. MRI showed an isointense mass on T1WI (Fig.1), arising from the clivus with extension into the sphenoid sinus, posterior ethmoid sinus bilaterally, left middle ethmoid sinus and nasopharynx. Mass was bulging into the prepontine cistern, causing flattening of the pontine bulge. Sellar floor was completely destroyed and pituitary gland was displaced superiorly and to the right side. Mass was also displacing the left cavernous sinus laterally. On T2WI, it was heterogeneously bright and showed homogeneous enhancement on gadolinium administration (Fig.2). With a preoperative diagnosis of clival chordoma, patient was operated via an extended frontobasal approach and near total excision of tumor was done. Tumor was greyish white, moderately vascular, firm with cystic areas containing dark yellowish fluid and dense hard calcified chunks pushing the sellar dura superiorly. Clivus was completely destroyed. There was no intradural extension of the tumor. A small part of the tumor was also invading the left cavernous sinus. Postoperatively, patient had hyponatremia and generalized tonic-clonic seizures which were treated appropriately. He was discharged on l2th postoperative day. The minimal left abducens paresis persisted. Postoperative CT scan confirmed complete excision of the tumor. Histopathological examination of tumor tissue revealed classical features of craniopharyngioma with characteristic adamantinomatous pattern (Fig. 3). Discussion Craniopharyngiomas are benign but aggressive neoplasms, that make up to 6% of the childhood intracranial tumors and 3% of all intracranial tumors.21 They are believed to arise along the path of the craniopharyngeal duct, which is the route taken by Rathke's pouch from the oropharynx to the floor of the third ventrincle. Craniopharyngiomas are most commonly located extra-axially in the suprasellar area (90%). However, approximately 18% of craniopharyngiomas extend into the sella and nearly 5% are purely intrasellar. They can extend to the anterior (2- 5%), middle (2%), or posterior (1-4%) cranial fossa. Infrasellar extension is found in about 5% of cases. Lesions in the ectopic locations are extremely rare. Rarely craniopharyngiomas arise primarily in unusual locations, such as nasopharynx,20 sphenoid bone.6,7,16 third ventricle,22 pineal gland,23 and cerebellopontine angle.24 Entirely infrasellar craniopharyngioma was first described by Bock in 1924,25 and was diagnosed at an autopsy. Since then, to the best of the authors' knowledge, 22 cases have been reported in the literature.1-18 Of the reported cases, most of them were intracranial with secondary downward extension, except two.19,20 The present case is unusual, as the entire tumor was lying extradurally in the infrasellar region occupying sphenoid sinus, ethmoid sinus, nasopharynx and was producing destruction of the clivus and mimicking a clival chordoma. In contrast to the suprasellar craniopharyngiomas, which usually present with complaints of visual disturbances, the infrasellar craniopharyngiomas present with nasal obstruction. In the present case, the patient did not have any symptoms related to nasal obstruction. There is no sex predilection for the infrasellar craniopharyngioma and majority of the reported cases presented in the third decade of life, in contrast to the suprasellar tumors which have slight male preponderance and the peak incidence is in the first two decades of life. Cyst formation and contrast enhancement is less common in infrasellar tumors as compared to suprasellar craniopharyngioma. In the present case, there was a small cyst, which was confirmed at surgery. These are slow growing benign lesions with a long standing history, and produce clival destruction and classically mimic a clival chordoma in this location. Similar findings were noted in this case also. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02054f1.jpg] [ni02054f2.jpg] [ni02054f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}