 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
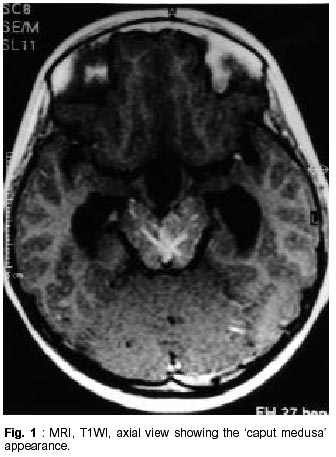
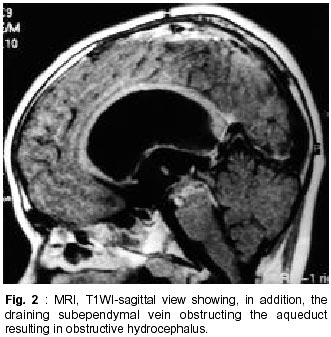
Neurology India, Vol. 50, No. 2, June, 2002, pp. 207-209 Midbrain Venous Angioma with Obstructive Hydrocephalus U. Bannur, I. Korah,* M.J. Chandy Departments of Neurological Sciences and Radiology*,
Christian Medical College and Hospital,
Vellore - 632 004, India. Accepted for publicaton : 30th November, 2001. Code Number: ni02057 Summary A rare case of a mid brain venous angioma with obstructive hydrocephalus is described. A dilated draining vein from the lesion in the aqueduct as the cause of the hydrocephalus is highlighted, and interesting features of the pathology of venous angiomas and associated cavernous hemangioma are described. The management of this interesting condition is discussed. Key words : Midbrain venous angioma, Hydrocephalus, CSF shunt. Introduction Although there have been a few references to venous angiomas in the brain stem, their occurrence in the midbrain with obstruction of the CSF pathway by a draining vein in the aqueduct is indeed rare. The pathology of these lesions make them unsuitable for surgical excision and therefore a CSF diversion procedure was carried out in the reported case with satisfactory result. Case Report An eleven year old boy was admitted to the neurosurgery ward with occipital headache of five months duration. Although the pain was dull and aching, there were two episodes of acute exacerbations. These exacerbations were associated with vomiting, vertigo and gait ataxia but they resolved on their own. There was no family history of neurological illnesses. On examination, the patient was normal on general physical review and neurological examination showed bilateral papilledema with no other positive findings. Image studies : CT scan, plain and contrast examination showed a 'spoke wheel' shaped lesion with one large vessel running ventrally into the posterior third ventricular region. There was no evidence of hemorrhage within or around the lesion. The lateral and third ventricles were dilated and the fourth ventricle was normal. MRI showed the 'caput medusa' within the mid brain, with multiple draining veins converging into a single vein, traversing the region of the aqueduct. This vein drained into subependymal veins and eventually into a dilated vein of Galen (Figs.1 and 2). Absence of CSF dynamic flow signals across the aqueduct confirmed the site of obstruction due to the dilated vein. The above findings were diagnostic of a venous angioma of the mid brain. Interestingly, there was no associated cavernous hemangioma. A CSF diversion procedure was then performed successfully. Discussion A venous angioma in the mid brain is rare and review of literature showed that the majority of these lesions were in other areas of the brain stem (Table I). Before the advent of CT and MRI, there have been postmortem reports of venous angiomas and a high incidence of vascular malformation upto 63%,1 and in a series of 168 posterior fossa vascular malformations, 11 venous angiomas were found in the brain stem.2 Earlier workers have made special mention of the angiographic features, especially of the venous system, in patients with venous angiomas. Venous angiomas were considered to be hamartomas by some some workers.3 Angiography, in patients with posterior fossa venous angiomas, showed absence of the normal venous anatomy. The drainage territories of the 'missing veins' were in fact drained by the radial veins of the angioma itself.4,5,1 The concept of anomalous venous drainage in these cases was however learnt after catastropic results following excision of a cerebellar venous angioma.1 This concept developed the hypothesis that these angiomas are part of an anomalous venous drainage of otherwise normal brain tissue and that these lesions are best left alone since attempted excision may lead to venous infarction and or brain edema. The spectrum of clinical presentation in patients with venous angiomas are varied even though the majority are incidentally found at autopsy or frequently seen on an MR study, more often than not in association with cavernous hemangioma. They rarely present as an ictus with subarachnoid or parenchymal hemorrhage, unless associated with cavernous hemangioma or as a progressive or fluctuating neurologic deterioration. The fluctuating course might simulate multiple sclerosis.6 The features of raised intracranial pressure and hydrocephalus have been described and have been ascribed to the marked dilation of the subependymal veins and consequent obstruction of the aqueduct.7-9 Craig and coworkers described a venous angioma in the basal ganglia with a draining vein adjacent to the aqueduct causing compression and obstruction to the CSF pathways.10 MR studies in the present case demonstrated CSF obstruction at the aqueduct due to a dilated subependymal vein. This is similar to the earlier observations of dilated subependymal veins providing an alternative venous channel in cerebellar venous angiomas.11 MR scanning is crucial to the diagnosis and subsequent management of venous angiomas. It is also useful in the assessment of hydrocepahalus and in the evaluation of other associated anomalies such as cavernomas and occasionally arteriovenous malformations.12 The role of digital substraction angiography is limited and can at best, document the associated anomalous venous drainage. Obstructive hydrocephalus due to a mid brain venous angioma is indeed rare and direct operative intervention is best avoided since it may lead to disastrous consequences. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02057f2.jpg] [ni02057f1.jpg] |
| |||||||||

{kind=link}
{kind=link}