 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
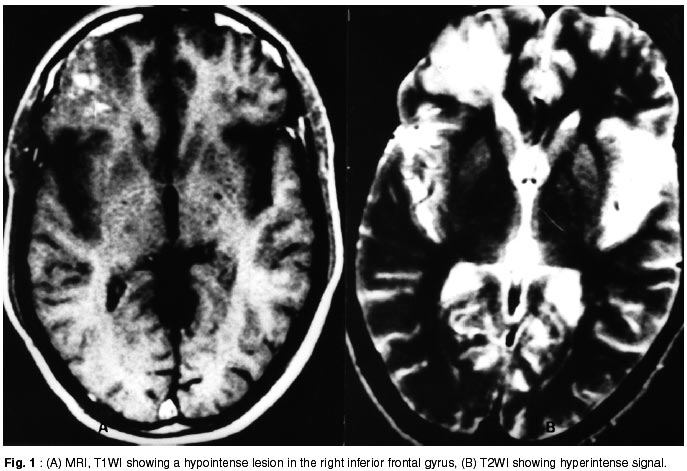
Neurology India, Vol. 50, No. 2, June, 2002, pp. 210-211 Short Report Unusual MR Presentation of Cerebral Parenchymal Tuberculosis R.T. Daniel, P.T. Henry, V. Rajshekhar Correspondence to : Dr. R.T. Daniel, Department of Neurological Sciences, Christian Medical College and Hospital, Vellore, Tamil Nadu, India. Code Number: ni02058 Summary The radiological abnormalities reported in CNS tuberculosis and their pathological correlates are discussed. Focal tuberculous involvement of the CNS without formation of tuberculoma is rare. The MR features in this case were also distinctly unusual for CNS tuberculosis. Therefore, histological confirmation of all lesions thought to be a low grade glioma is mandatory. Key words: Meningoencephalitis, Tuberculosis, Central nervous system. Introduction Tuberculosis of the central nervous system can present in various forms with meningitis and tuberculomas being the commonest. Basal contrast enhancement is a consistent feature of tuberculous meningitis on CT scan and MRI. Tuberculomas also show contrast enhancement on CT and MR imaging. Though it has been postulated that tuberculomas in the cerebritis stage may be seen as areas of hypodensity without enhancement on CT scans, this hypothetical picture has never been documented by histological examination. Case Report A 46 year old male presented with non-progressive headache, with no other features of raised intracranial pressure, of 18 months duration. He also had two episodes of loss of consciousness suggestive of generalized seizures. Clinical examination revealed normal fundi, pronator sign in the left upper limb and impaired foot tapping in the left lower limb. CT scan showed mild asymmetry of the frontal horn on the right side. MRI showed an ill-defined lesion in the right inferior frontal gyrus, which was hypointense on T1WI and hyperintense on T2WI (Fig. 1), with areas of patchy enhancement with gadolinium. There was no mass effect or perifocal edema. Clinical and radiological possibility of a low grade glioma was considered. Due to the non-progressive nature of the disease, and the radiological picture of a wedge shaped hypointensity, the possibility of an infarct was also considered. He underwent a right frontal craniotomy and radical excision of the lesion. The mass was of rubbery consistency and not suckable. Believing that it was a low grade glioma, the mass was radically excised up to the ventricular wall. Histopathological examination of the specimen showed a dense infiltration of lymphocytes and few plasma cells around focal small aggregates of epithelioid cells and Langhans type giant cells. There was extension of these cells into the adjacent nervous parenchyma along with spongiosis and reactive gliosis in the surrounding neural tissue, which was reported as tuberculous meningoencephalitis. He was given a four drug anti-tuberculous chemotherapy for 18 months. At follow up (after chemotherapy), he was found to be asymptomatic and had no neurological deficits. Contrast enhanced CT scans showed no evidence to suggest any residual or recurrent disease. Discussion Meningitis is a common manifestations of CNS tuberculosis. Most of the pathological changes in this condition are in the meninges. However, parenchymatous involvement along with meningitis, either due to direct involvement or secondary to vascular changes, is often seen.1 Thus, pathologically, tuberculous meningitis is truly a meningoencephalitis. The brain may be involved to varying extent. Two types of parenchymatous involvement have been described i.e. border zone reaction and infarcts/ischemic lesions.2 In the former case, whenever the brain comes into contact with the tuberculous exudate, there is a concurrent inflammatory response. There are, consequently, varying degrees of edema, perivascular response and microglial reaction. In the long-standing case, there is in addition, significant gliosis. Similar to the submeningeal region, the subependymal region is also a border zone and hence shows similar changes.2 In cases of meningitis, there is 'en plaque' meningeal thickening on plain CT, mainly in the basal cisterns. Contrast administration reveals abnormal meningeal enhancement. It has been postulated that tuberculomas, during the acute stage (cerebritis stage), may appear as hypodense areas on the CT scan. However, this hypothetical picture on CT has never been correlated with a histological examination.3 Tuberculomas may be isodense or slightly hyperdense on plain scans. On administration of contrast, based on the pattern of enhancement, tuberculomas fall into 3 distinct categories : i) solid enhancing lesions, ii) ring enhancing lesions, and iii) mixed or combined forms of lesions.3 Mature tuberculomas are well delineated round or oval ring enhancing masses.4 Sometimes, they appear as a ringenhancing lesion with a central area of enhancement or calcification ('target sign').4 MRI, however, does not reveal any meningeal change on plain scans. Gadolinium administration shows basal meningeal inflammatory pattern, similar to that seen on CT, on the T1WI. Tuberculomas are typically isointense to brain on T1WI with marked enhancement on contrast administration.5 On T2WI, they have central hyperintensity and a hypointense rim. Hypointense images on T2WI are associated with increased fibrosis, gliosis and macrophage infiltration.6 In the present case, there was no evidence of exudates in the subarachnoid space at surgery. The arachnoid also appeared normal. Both histologically and radiologically, this is unusual. Pathologically, focal tuberculous involvement of the cerebral parenchyma without the formation of a tuberculoma is distinctly rare. The unusual lack of significant gadolinium enhancement is also very atypical for tuberculous process. Tuberculous involvement of the parenchyma is usually associated with significant enhancement. The MR changes (hypo- to isointense on T1WI and hyperintense on T2WI) in our patient are possibly due to the spongiosis and reactive gliosis in the brain. There were no pathological changes of ischemia which could explain the MRI. Finally, this case also underlines the need for histological verification of low grade gliomas, suspected on imaging. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02058f1.jpg] |
| |||||||||

{kind=link}