 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
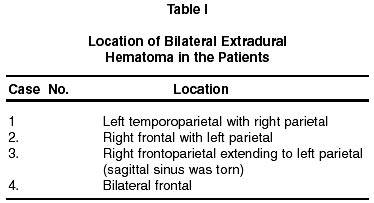
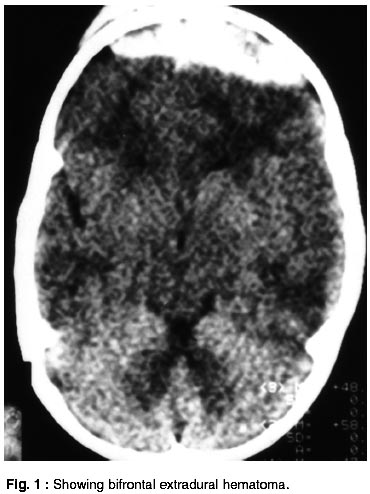
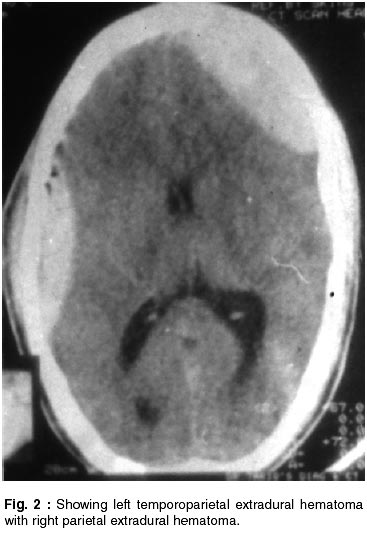
Neurology India, Vol. 50, No. 2, June, 2002, pp. 217-218 Short Report Acute Bilateral Extradural Hematomas A. Ramzan, A. Wani, A.H. Malik, A. Kirmani, M.A.Wani Correspondence to : Dr. A. Ramzan, P.O. Box 974, G.P.O., Srinagar 190 001, Kashmir, India. E-mail : drauramjan@usa.net Code Number: ni02061 Summary The occurrence of bilateral extradural hematomas is an uncommon consequence of craniocerebral trauma and its incidence is variable in various studies ranging from 2-25%.1 We studied all cases of head injury brought to our institute over a period of 6 months and found the incidence of bilateral extradural hematomas to be 13.3%. Key words: Extradural hematoma, Trauma, Evaluation. Introduction Extradural hematomas are one of the modes of presentation of head injury. Usually, they are unilateral, often occurring in middle meningeal artery territory. Most of these cases demand urgent surgical intervention, aiming at their evacuation. In some cases, there is bilateral occurrence of these extradural hematomas. They are all the more dangerous unless quick evacuation is done. We studied these cases regarding their evaluation, location, clinical profile and outcome. Material and Methods A retrospective analysis of 30 cases of extradural hematomas, operated over a period of 8 months was done. Four cases had bilateral extradural hematomas. All patients were evaluated by non contrast CT scan. Location of extradural hematoma varied (Table I). Surgical evacuation was done in all cases by conventional methods. One patient was in the pediatric age group while others were adults. Two patients (adults) had GCS of 14 and 15 and third adult had GCS of 8 at the time of admission. In first two cases GCS at time of discharge was 15 while in third cases GCS was 12 at time of discharge. Fourth patient (pediatric) had GCS of 7 at time of admission which fell later on (Table II). Road traffic accidents were responsible in 50% of cases, the remaining 50% cases being due to domestic fall. Results and Discussion Incidence of bilateral extradural hematomas has been variably reported in various studies, i.e. ranging from 2-25%.2-6 In the present study, it was 13.3% during the period this study was conducted. Two of our patients had preoperative GCS of 14 and 15 which continued to be so in postoperative period. In third case, it was 8 at the time of admission and 12 at the time of discharge. In fourth case, it was 7 at the time of admission, but fell to 4. The fourth case had bilateral chest signs and acute respiratory distress syndrome (ARDS); he had to be kept on ventilator, but ultimately the patient died. In all the cases, fracture skull was present. In two of our patients no focal neuro deficit was present at the time of admission, while the third case had bilateral dilatated of pupils. In fourth case pupil inequality was seen. All of our patients were subjected to evacuation of hematoma. Three of our patients had bifrontal hematoma alone (Fig. 1). Only one case had hematoma in frontoparietal and contralateral parietal region (Fig. 2). All the patients were operated within 48 hours of sustaining injury. Various theories have been put forward, regarding mechanism of occurrence of bilateral hematomas. It has been suggested that dura is detached from two locations by a single directed force. Stripping of dura can occur at site of impact by inbending or outbending of skull7 or due to motion of skull, further aggravated by the negative intracranial pressure found at the antipode of the compression force.8 In bilateral hematomas direction of force tends to be anteroposterior rather than lateral,7 besides it can also occur due to extension of fracture line across midline, leading to bilateral extradural hematomas under fracture line, as was seen in one of our cases (Fig. 1). It has also been suggested that the mechanism is same as in the coup and contre-coup injuries.9 Two of our patients had good recovery and returned quickly to normal routine life, while one had mild disability with hemiparesis (but patient still could walk with mild support) and one died. These results are comparable to some of the earlier reported studies. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02061t1.jpg] [ni02061t2.jpg] [ni02061f2.jpg] [ni02061f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}