 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
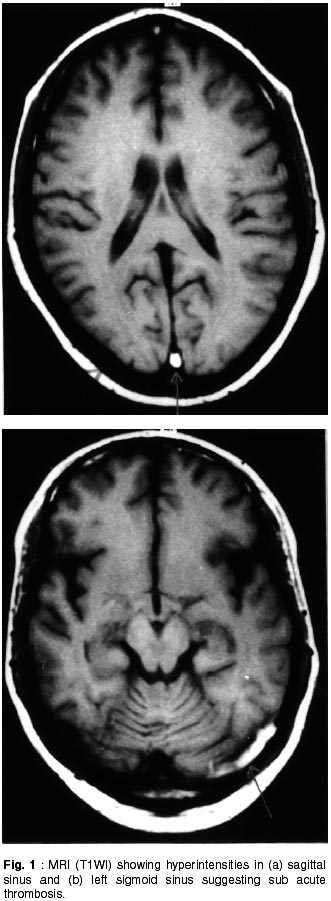
Neurology India, Vol. 50, No. 2, June, 2002, pp. 215-217 Short Report Cerebral Venous Thrombosis in Ulcerative Colitis A.K. Srivastava, N. Khanna, V. Sardana, S. Gaekwad, K. Prasad, M. Behari Correspondence to : Dr. M. Behari, Professor and Head, Department of Neurology, Neurosciences Centre, All India Instiute of Medical Sciences, New Delhi - 110 029, India. Code Number: ni02062 Summary Cerebral venous thrombosis is a rare complication of ulcerative colitis. We report a case of 29 year old male who developed superior sagittal, left lateral and sigmoid sinus thrombosis secondary to ulcerative colitis. He was successfully treated with low molecular weight heparin and steroids. Key words: Ulcerative colitis, Cerebral venous thrombosis, Low molecular weight heparin. Introduction The occurrence of thrombosis in both venous and arterial systems has been recognized for over 60 years as a distinct complication of ulcerative colitis.1-4 Cerebral venous thrombosis (CVT) is a less common but potentially fatal complication with only few cases reported in the world literature.5-7 It occurs most commonly in the setting of active disease and its outcome is poor with more than 80% cases developing permanent sequel or death. The precise mechanism involved in thrombogenesis remains unclear and the treatment remains controversial. We report a case of cerebral venous thrombosis in a patient with ulcerative colitis, treated with corticosteroids, low molecular weight heparin (LMWH), mannitol and acetezolamide. The patient improved completely. Case Report A 29 year old man developed recurrent bloody loose motions and after detailed investigations, which included a colonoscopy and colonic biopsy, was diagnosed to have ulcerative colitis. His symptoms improved with 5-aminosalycillic acid and steroids. He was admitted with complaint of sub-acute onset global headache and vomiting, six months after the onset of gastrointestinal symptoms. His headache worsened over next few days, vomiting became more frequent and he developed diplopia. He developed sudden onset left facio- brachial paresis 10 days after the onset of headache. Neurological examination revealed bilateral papilledema, bilateral 6th nerve paresis, left upper motor neuron facial paresis and mild (grade 4/5) weakness of left upper limb. Deep tendon reflexes in left upper limb were slightly diminished with bilateral flexor plantar responses. He had hemoglobin of 14 gm%, total leukocyte count of 11,300/mm3 with normal differential counts and platelet count of 2,20,000/mm3. Erythrocyte sedimentation rate (ESR) was 25 mm in 1st hour (Westergren). Routine biochemical parameters were normal. Coagulation profile including prothrombin time (PT), partial thromboplastin time (PTT), protein C and protein S were normal. Antinuclear antibodies, rheumatoid factor, anticardiolipin antibodies and lupus anticoagulant were negative. Examination of cerebrospinal fluid revealed 2 lymphocytes/mm3 protein 80 mg% and sugar 116 mg% (blood sugar 146 mg%). Non contrast computerized tomographic scan (NCCT) of head, after onset of headache and after 12 hours of onset of facio- brachial weakness was normal. MRI and MR venography (MRV) showed absence of normal flow void in superior sagittal, left lateral and sigmoid sinuses. Hyperintensities were noted in both T1WI (Fig. 1) and T2WI within these dural sinuses, suggestive of sub acute thrombosis. He was given intra venous dexamethasone and mannitol. Subcutaneous low molecular weight heparin was given in doses of 0.4 ml (40 mg) 12 hourly after the onset of left facio-brachial paresis, and was continued for 21 days. His weakness started improving after 3 days and improved completely in two weeks. Headache and 6th nerve paresis improved completely in one week and later papilledema also improved. Follow up MRI and MRV after 3 weeks showed similar hyperintensities as seen in previous MR study but there was evidence of partial recanalization in torculae and posterior superior sagittal sinus. No parenchymal abnormalities were found on both MR studies. Discussion Bargen and Barker reported extensive thrombosis of blood vessels as a serious complication of ulcerative colitis.1 The incidence of this complication in clinical studies varies between 1.2 to 7.5%. However, in autopsy studies a high incidence of 32 to 39% has been reported.3,4 The variation could be due to difficulty in detecting CVT during life or due to occurrence of CVT, mostly towards the terminal stage of ulcerative colitis. The thromboembolic complications of ulcerative colitis are now being increasingly identified, owing to the development of a variety of intracranial imaging techniques.7 Primary cerebral venous thrombosis is not associated with trauma, intracranial procedure, paranasal sinus infections and otitis media.5 Commonly anemia, dehydration, low cardiac output and alterations in blood coagulability combine to precipitate this complication in an already ill patient. Primary cerebral venous thrombosis is rare in young adults. In two review articles, consisting of a total of 118 cases of CVT, none was attributable to inflammatory bowel disease.8,9 CVT occurs in association with autoimmune conditions (immune thrombocytopenic purpura, systemic lupus erythematosus, hemolytic anemia), coagulation abnormalities (thrombocytosis, deficiency of protein C, protein S and antithrombin III), red blood cell (RBC) abnormalities (polycythemia, sickle cell anemia), cryofibrogenemia and paroxysmal noctural hemoglobinuria. Other conditions like pregnancy and puerperium, congestive heart failure, shock, dehydration, diabetic ketoacidosis, oral contraceptives: metastatic tumors, hyperlipidemia, homocystinuria and sepsis have also been found to be associated with primary cerebral venous thrombosis. The etiology of hypercoagualability and thromboembolism in ulcerative colitis remains obscure.5 During active state in ulcerative colitis, association of coagulation factors and platelet abnormalities are well documented. Thrombocytosis and elevated fibrinogen level, factor V, factor VIII and decreased antithrombin III have also been described in active stage of ulcerative colitis. Deficient platelet aggregation, increased thromboplastin generation and the presence of fibrin microclots have been implicated. There is no substantial evidence to implicate hematological and coagulation abnormalities in thrombogenesis.5 Out of 16 cases of cerebral venous thrombosis associated with ulcerative colitis in a review, only 4 had abnormal coagulation profile i.e. antithrombin III deficiency, mild thrombocytosis and elevated factor VIII with mildly decreased PTT in another.5 One patient had elevated levels of factor V, VIII and XI and protein C. In the present case also, coagulation studies were within normal limits. There are no established guidelines for management of CVT in ulcerative colitis.5 Role of heparin is controvertial. Surgical thrombectomy and peripheral thrombolytic therapy by local infusion of urokinase or streptokinase by a trans-jugular or direct intracranial sinus approach have been tried. However, none of the patients reported had been given low molecular weight heparin (LMWH), which has been advocated both as a prophylactic and therapeutic agent for preventing venous thromboembolism.10 It has longer plasma half-life, better bio-availability and is associated with lower hemorrhagic risk, as compared to heparin, while having similar antithrombotic activity. In view of above reasons, LMWH was chosen, in present case during three weeks of LMWH therapy, there was, no bleeding complication. Dexamethasone, mannitol and acetazolamide were also used. Patient was put on low dose aspirin at discharge. During follow up, headache decreased and papilledema disappeared. Steroids were gradually tapered off over six weeks. To the best of our knowledge this case is probably the first case of cerebral venous sinus thrombosis secondary to ulcerate colitis that was treated successfully with LMWH. The case also reflects the rare occurrence of CVT in ulcerative colitis. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02062f1.jpg] |
| |||||||||

{kind=link}