 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
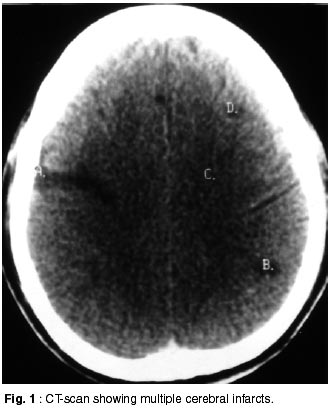
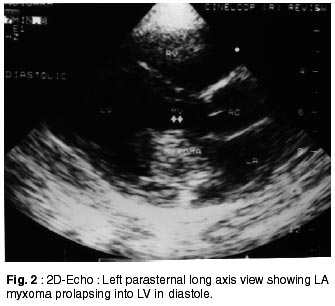
Neurology India, Vol. 50, No. 2, June, 2002, pp. 219-220 Short Report Left Atrial Myxoma Presenting as Pseudobulbar Palsy A. Kumar, A. Sachdev, R. Singh, S.S. Lehl, S. D'Cruz, M. Mahapatra, H.S. Malhotra Correspondence to : Dr. A. Kumar, Department of Medicine, Government Medical College and Hospital, Sector - 32B, Chandigarh - 160 047, India. Code Number: ni02063 Summary A case of left atrial (LA) myxoma presenting as pseudobulbar palsy, due to multiple cerebral infarcts, without any cardiac manifestations, is presented. LA myxoma is rare cause of embolization to CNS causing ischemic infarcts. Due to multiple CNS infarcts patient can present with varied clinical picture and pseudobulbar palsy is not a very common presentation. It was a real diagnostic dilemma before LA myxoma was diagnosed on echocardiography. Key words: Left atrial myxoma, Multiple cerebral infarcts, Pseudobulbar palsy. Introduction Primary cardiac tumors are found in 0.05% of routine autopsies and are a rare cause of cerebral emboli. Myxomas are the most common of these tumors and constitute nearly 50% of all tumors of the heart and about 75% of them occur in the left atrium.1 The triad of obstruction, embolization and constitutional manifestations may suggest the diagnosis of left atrial myxoma, but cardiac imaging studies are usually required since clinical evaluation rarely discloses specific findings.2 Systemic embolization of tumor fragments has been reported in 60% of patients with left atrial myxomas.3,4 The symptoms cannot be distinguished from acute arterial insufficiency of other etiologies. We describe a case who presented with features of pseudobulbar palsy because of multiple CNS emboli from left atrial myxoma. Case Report A 38 years old male presented with symptoms of difficulty in speaking, weakness of lower limbs, crying and laughing without any reason and perioral twitching for the last 2 months. Three months back, the patient had transient weakness of right half of the body and two episodes of seizures. There was no history of dysphagia, nasal regurgitation, diplopia or bowel or bladder incontinence. Patient was not a diagnosed case of hypertension, diabetes mellitus, ischemic heart disease or rheumatic heart disease. Initial examination revealed emotional lability and spastic speech. Cranial nerve examination was normal. Motor examination revealed hypertonia with power of grade IV/V in all the four limbs, hyperreflexia and brisk jaw jerk. His plantars were mute. There were no cerebellar signs and gait was normal. Sensory system examination was normal. Cardiovascular system examination was also normal. Investigations revealed raised ESR of 60 mm in Ist hour; blood chemistry and lipidogram were within normal limits. ECG demonstrated sinus rhythm with atrial ectopics. Chest X-ray and X-ray cervical spine were normal. RA factor and ANF were negative. CTscan revealed focal rounded and linear hypodense areas without any contrast enhancement, in both parietal regions, mainly subcortical and cortical in locations and in peripheral parts of left cerebellar hemisphere (Fig. 1). Echocardiography revealed a large myxoma attached to inter atrial septum (size- 3.38x3.42 cm), which was prolapsing into left ventricle during diastole (Fig. 2). With this, a final diagnosis of left atrial myxoma presenting as pseudobulbar palsy was made because of multiple CNS infarcts. Discussion 15% of all ischemic infarcts occur due to embolism from the heart and atrial myxoma accounts for only 0.5% of them.5 Most cardiac myxomas occur in left atrium. Majority of these are attached to atrial septum near the fossa ovales, may be pendunculated or sessile; and 90% are solitary.6 The friable, pedunculated and polypoidal type tumors are more likely to embolize because of their mobile nature and the embolic material can be either thrombus or actual tumor fragments.7,8 Tumor emboli have been noted at virtually all systemic locations but cerebrovascular embolization occurs most often.9,10 The fate of the tumor fragment, which embolizes to the cerebral vessel within the CNS remains controversial.11 Two late complications have been reported - either tumor fragment may grow and present as expanding intracranial mass or there may develop a vascular aneurysm at the site of embolus.11 In our patient at present only areas of infarctions have been picked up on cranial CT in territory of middle cerebral artery and in vertebro-basillary circulation. Clinical picture of pseudobulbar palsy can be seen in various clinical settings like : amyotrophic lateral sclerosis, multiple sclerosis and multiple CNS infarcts, causing disruption of corticobulbar tracts. Our patient developed pseudobulbar palsy due to multiple CNS infarcts. This case illustrates that in patients with recurrent embolic events leading to multiple CNS infarct, with clinical picture of pseudobulbar palsy without cardiac symptoms or signs, cardiac myxoma, though rare but treatable cause, must be considered as a source of embolization. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02063f2.jpg] [ni02063f1.jpg] |
| |||||||||

{kind=link}
{kind=link}