 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
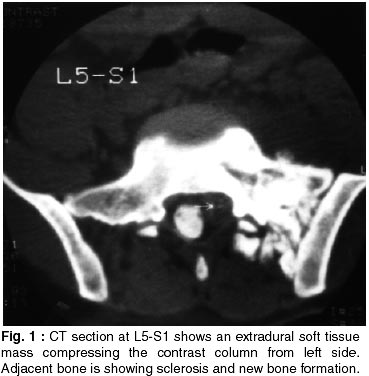
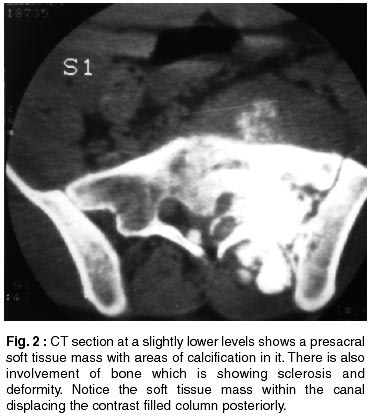
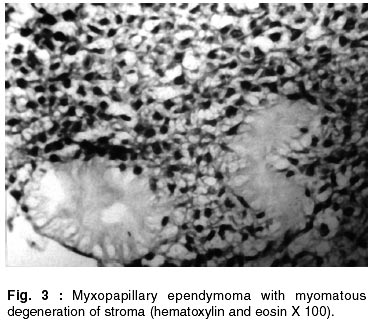
Neurology India, Vol. 50, No. 2, June, 2002, pp. 223-224 Extradural Ependymoma with Extraspinal Extension : Letter to Editor S. Magu, T.S. Jaswal,* D.S. Mishra, N.K. Magu,** P. Popli, N. Sharma Department of Radiology, Pathology* and Orthopedics,** Pt. B.D. Sharma Postgraduate Institute of Medical Sciences, Rohtak - 124 001, Haryana, India. Code Number: ni02066 Ependymomas are the most common glial tumors of conus medullaris, filum terminale and cauda equina.1 Ependymomas have also been reported in the extraspinal soft tissues of the sacral region, producing bone deformity and growing to great size.2 These extraspinal ependymal tumors are thought to be congenital in origin.1 We report a case of myxopapillary extradural ependymoma with extraspinal extension in presacral region in a 17 year old male presenting with weakness of the left lower limbs. A 17 years old male was admitted with the complaints of backache and limping. He gave history of fall from the stairs one and a half year back. On examination, there was weakness of the left lower limb. Plain X-ray of the lumbosacral spine showed sclerosis of left sacral ala. Myelography showed cutting off of the nerve roots at the level of L5 on the left side. Myelo CT at L5 showed a soft tissue mass within the spinal canal causing pressure effect on the contrast column on left side, involving the nerve roots (Fig. 1). CT at a slightly lower level showed bone involvement with sclerosis and extension into the soft tissues with areas of calcification (Fig. 2). On histopathology, the lesion was a myxopapillary ependymoma (Fig. 3). The tumor was infiltrating the bone as well. About 60% of glial tumors in the spinal canal are ependymomas.3 Approximately, 60% of ependymomas occur along the course of the filum terminale in adults. There is fairly even distribution in age from 20 to 60 years. Males are slightly more affected than females.1 Clinical presentation is usually a combination of lower extremity weakness, occasional pain, bowel and bladder disturbance and rarely subarachnoid hemorrhage or hydrocephalus. Spinal cord ependymomas arise from the ependymal cells lining the central canal or its remnants in filum terminale.3 Extradural ependymoma is a rare tumor, arising most commonly in the presacral area, less commonly in the soft tissue of sacrococcygeal region, dorsal to the sacrum and rarely in the extradural portion of spinal canal. The differential diagnosis varies with the location of tumor, but natural history of tumor is the same. The tumor may recur if not completely excised at surgery.4 Ependymomas are slow growing tumors and often reach a relatively large size before becoming symptomatic.1 Various variants of ependymomas include ependymoblastoma, myxopapillary ependymomas, papillary ependymomas and subependymomas.5 Myxopapillary ependymomas can occur throughout the cerebrospinal axis; even in the hollow of the sacrum. It is far more frequent at the level of cauda equina. However, infrequently the tumor in seen to arise in the hollow of the sacrum, when it is necessary to distinguish it from poorly differentiated teratoma.3 Upto 20% of cases metastsize, often after a very prolonged latent period.6 In the myxopapillary type, the vascular and connective tissue undergo great degree of myxoid change.3 Plain X-ray usually shows erosion of neural arch, pedicles or vertebral bodies. Non contrast CT shows an isodense to hypodense mass, enhancing on intravenous contrast. While calcification has been reported in posterior fossa and supratentorial ependymomas, it is not commonly seen in spinal cord ependymomas.1 The ependymomas of cauda equina appear as a centrally placed spherical mass. The nerve roots of cauda equina above and below the tumor mass can be identified and conus can be demonstrated separate from the mass on post myelographic CT. Intramedullarly ependymomas arising in thoracic and cervical region are not distinguishable from astrocytomas by myelography, intrathecal contrast CT, contrast enhanced CT or MRI. Ependymomas can also arise in extraspinal soft tissue of sacral region, producing bone deformity and growing to great size2 as in the present case. They are of myxoid papillary type and are thought to arise from coccygeal medullary vestige, and ependymal lined cavity in caudal portion of neural tube that lies beneath the skin of post natal pit. Spina bifida may be associated. These extraspinal tumors are thought to be congenital in origin. MRI shows these lesions to be slightly hypointense on T1WI and hyperintense on T2WI.1 References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02066f2.jpg] [ni02066f1.jpg] [ni02066f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}