 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
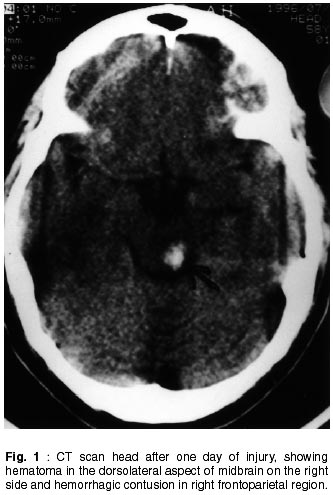
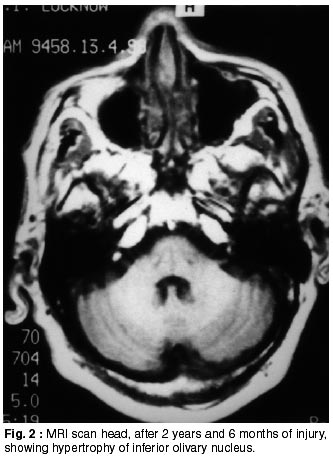
Neurology India, Vol. 50, No. 2, June, 2002, pp. 222-223 Palatal Myoclonus Following Head Injury : Letter to Editor B. Bansal, P. Singh, R. Shukla Department of Neurology, King George's Medical College, Lucknow - 226 003. U.P., India. Code Number: ni02068 Since its first description in 1962, palatal myoclonus (PM) has been recognized as a distinct and rare clinical entity characterized by recurrent rhythmic contraction of soft palate, which may be accompanied by contraction of larynx, pharynx, diaphragm or extraocular muscles.1 It usually develops secondary to a residual lesion of CNS, and is consequently termed symptomatic, while patients with no evidence of structural lesion of CNS are labelled as essential myoclonus.2 There are infrequent case reports from India.3 We report a case of palatal myoclonus secondary to post-traumatic intracerebral hemorrhage. A 60 years old right handed engineer became unconscious after a road traffic accident, two and half years back and was admitted to a local hospital. The GCS scale was 6 (E1V1M4) and left sided hemiparesis was present. CT scan head showed a hematoma (0.4 x 0.7 cm) on right side of midbrain, on dorsolateral aspect and hemorrahagic contusion in right frontoparietal region (Fig. 1). The patient was treated conservatively and he regained consciousness after 36 hours. MRI scan two weeks after injury showed hyperintensities on T2WI on right side of midbrain and in right frontoparietal region. After discharge, the patient noticed intention tremor in left upper limb which gradually increased in severity within 12 months along with rest tremor. Six months later, he developed difficulty in writing and intention tremor in right upper limb also. Patient was a known diabetic since 1983. On examination in April 1999, his pulse and blood pressure were normal. Speech was dysarthric. Cranial nerve examination revealed bilateral rhythmic symmetrical palatal movements occuring at a rate of 130/minute (the patient was unaware of it and there was no ear clicking). Motor system examination revealed power of 4+ to 5 on left side. Deep tendon reflexes were normal and plantar responses were flexor bilaterally. Sensory system examination showed impaired vibration sense at both ankles. Bilateral cerebellar signs (left > right) were present. Patient also had left head tremor (titubation) at a rate of 130/minute. All routine investigations including brainstem auditory evoked responses from both the ears were normal. A repeat MRI scan showed a hyperintense lesion on T2WI on right side of midbrain and gliosis in right frontal region with increased T2 signal intensity and hypertrophy of the inferior olivary nucleus bilaterally (Fig. 2). Patient was diagnosed as a case of symptomatic palatal myoclonus and put on clonazepam 0.5 mg orally three times a day, in addition to the antidiabetic treatment. Follow-up after three months did not show any improvement. The common causes of palatal myoclonus include cerebrovascular disease, multiple sclerosis, tumors, trauma, infection, Behcet's disease and vertebral artery aneurysm.4 Primary (idiopathic) PM occurs in younger age group (30-40 years) with equal distribution in both sexes, has lower frequency and can be affected by sleep, coma and anesthetics. It usually presents with ear clicks. Secondary PM occurs in older age group (40-60 years), is more common in males, not affected by sleep and does not cause any symptom.2 PM after infarction of the brainstem or cerebellum is due to denervation supersensitivity secondary to lesions involving the dentato-rubroolivary system. The interval varies from 2 to 49 months with the median between 10 and 11 months. Ultrastructural changes in the form of granulovacuolar degeneration and chromatolysis have been observed.5 Abnormalities in serotonergic, cholinergic, glutamate and opioid neurotransmitter may be the neurochemical basis of PM. PM is markedly resistant to treatment. Trihexiphenidyl, clonazepam, sumatriptan, flunarizine, 5-hydroxytryptophan in combination with carbidopa and carbamazepine have been reported to be beneficial in some cases. Botulinum toxin may be the latest addition to the armamentatrium of drugs used in treatment of PM. Spontaneous recovery has been rarely reported. In the present case head injury leading to hematoma in right midbrain was responsible for rubral tremor and PM, developing 10 months after the head injury. The interesting feature was the occurence of left upper limb and head tremor and PM at the same rate. Movements of extremity such as myoclonus or tremor is uncommon in PM. Five patients with palatal myoclonus and rest tremor were reported by Masucci and Kurtzke.6 In four patients, a slow rest tremor (3 Hz or less) was present. The tremors persisted on sustained posture and finger to nose manoeuvers and was usually not synchronous with palatal movements. The presence of right sided cerebellar signs in the patient is an interesting finding which has not been reported earlier. This may be explained due to post traumatic cerebellar degeneration. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02068f1.jpg] [ni02068f2.jpg] |
| |||||||||

{kind=link}
{kind=link}