 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 235-237 Editorial Spasticity M. Behari Department of Neurology,
All India Institute of Medical Sciences,
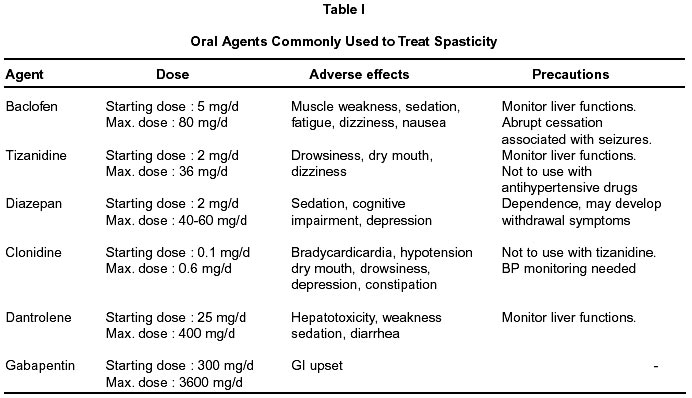
Ansari Nagar, New Delhi - 110 029, India. Code Number: ni02074 Almost a century ago, Sherrington transected a cat's brain stem above the vestibular nucleus and produced an animal with increased stretch reflexes and tone in antigravity extensor muscles.1,2 This was said to be 'decerebrate rigidity'. Although animal decerebrate rigidity is not considered analogous to human spastic states, Sherrington's seminal study of cat's myotactic stretch reflex established a model of an afferent - efferent neural circuit and paved way for better understanding of spasticity. Nathan described spasticity emphasizing the central role of stretch reflex. In his land mark paper he wrote 'spasticity is a condition in which stretch reflexes that are normally latent become obvious. The tendon reflexes have a lowered threshold to tap, the response of the tapped muscle is increased, and usually muscles besides the tapped one respond; tonic stretch reflexes are affected in the same way'.3 Frequently cited definition proposed by Lance states 'spasticity is a motor disorder characterized by a velocity dependent increase in tonic stretch reflexes (muscle tone) with exaggerated tendon jerks, resulting from hyper excitability of the stretch reflexes, as one component of the upper motoneuron syndrome'.4 Work of Sherrington and others defined an afferent - efferent model of stretch reflex and the role of proprioceptive, exteroceptive and descending supraspinal inputs such as reticulo-spinal, rubro-spinal and vestibulo-spinal afferent in the pathogenesis of spasticity. Role of alpha-motoneurons and inhibitory Renshaw interneurons in spasticity is well known. Though the phasic reflex arc is dependent on tendon lengthening and excitatory post synaptic potentials (EPSPs) carried by I-a afferents, inhibitory post synaptic potentials (IPSPs) arising from antagonistic muscle spindles, oligosynaptic and polysynaptic pathways also have important role in maintenance of tone.5-7 Spasticity results from prolonged disinhibition of components of this system. Damage to pyramidal tracts alone whether in the cortex, cerebral peduncle, basis points or medullary pyramids does not result in spasticity. It is only when lesions involves premotor and supplementary motor areas that the spasticity occurs. Neurologists are faced with several situations where spasticity is responsible for major disability. Some of these situations are stroke, trauma, degenerative disorders, multiple sclerosis and cerebral palsy in children. Before treatment is begun the goals of therapy should be clearly identified. The main goal of therapy is to increase functional capacity and relieve discomfort. The consequences of reduction of spasticity should be assessed. If spasticity offers stability to a joint and acts as props for limbs, its reduction may only jeopardise the patients functional capacity. On the other hand, if there is minimal weakness with predominant spasticity treatment of spasticity will result in tremendous improvement in functional capability. Non ambulatory patients with moderate to severe weakness, hyperflexia, clonus and painful flexor spasms interfering with hygiene and nursing require treatment of spasticity. However, the goal of therapy should be very clear to the physician, the patient and the care giver. Physical therapy along with antispasticity drugs and surgical therapy remain the corner-stone in the management of patients with spasticity. Among the pharmaco-therapeutic agents baclofen, a GABA analogue,8-10 tizanidine an imidazole derivative and a centrally acting á2 adrenergic agonist,11-13 diazepam,14 clonidine a centrally acting a-2 adrenergic agonist,15 dantrolene a hydantoin derivative inhibiting the release of Ca++ from sarcoplasmic reticulum thus interfering with excitation - contraction coupling,16,17 gabapentin a GABAergic agent18 and botulinum toxin which acts by preventing release of acetylcholine at the neuromuscular junction thus providing chemodenervation19- 21 have shown promise. All these agents except clonidine and gabapentim have shown significant efficacy in the management of spasticity. Among these drugs baclofen and tizanidine have similar efficacy and recommended first line treatment in Indian setting. Less weakness and more night time insomnia reported with tizanidine as compared to baclofen make both equal in side effect profile. When the dose of oral anti - spasticity drugs is high and spasticity is severe and generalized, intrathecal delivery of baclofen through a pump implanted in the abdominal wall with a catheter threaded into subarachnoid space provides 4 times the concentration of drug at only 1% of the oral dose.22,23 The cost of the implant in India is approximately 2.5 lac rupees and the recurrent cost of baclofen is Rs. 3000-4000 which lasts anywhere from 3 to 4 months. On the more invasive side, nerve blocks with phenol and alcohol provide relief from especially in children with spastic cerebral palsy (CP).24 Other surgical procedures such as tenotomy, tendon lengthening, tendon transfer and selective dorsal rhizotomy25 are some of the procedures especially useful in children with CP with good muscle power. Myelotomy though performed rarely is associated with loss of control of bowel and bladder, strength and sensation. Spinal cord stimulation currently used more for pain reduction may prove to be clinically effective in reduction of spasticity in future. Understanding of pathogenesis of spasticity has improved since it was first described by Sherrington. Development of medical technologies, new pharamoco-therapeutic agents and drug delivery system have improved the quality of life for many patients of spasticity. Availability of a wide array of therapeutic options has increased the responsibility of the physician in deciding the option best suited to a given patient. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02074t1.jpg] |
| |||||||||

{kind=link}