 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 244-255 Views and Reviews Neuronavigation : Concept, Techniques and Applications O. Ganslandt, S. Behari,* J. Gralla, R. Fahlbusch, C. Nimsky Department of Neurosurgery,
University of Erlangen-Nuremberg,
Schwabachanlage 6, 91054, Erlangen, Germany
and
Department of Neurosurgery*
Sanjay Gandhi Postgraduate Institue of Medical Sciences,
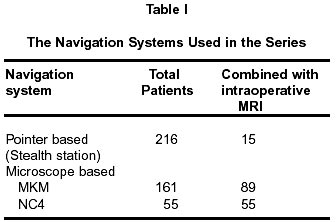
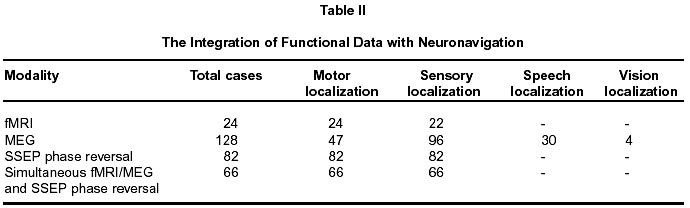
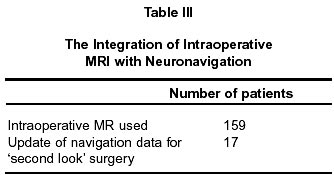
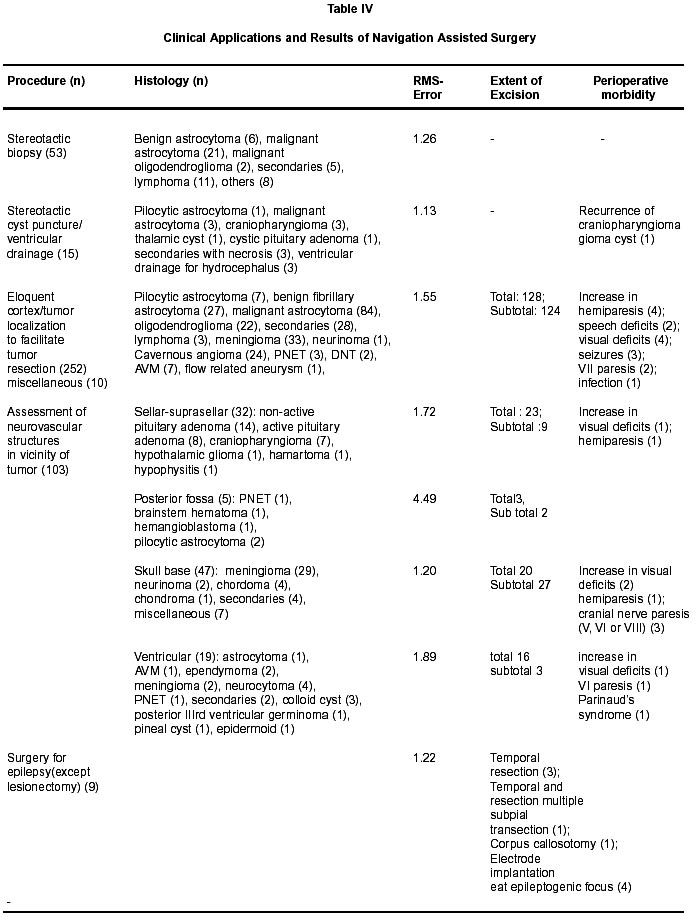
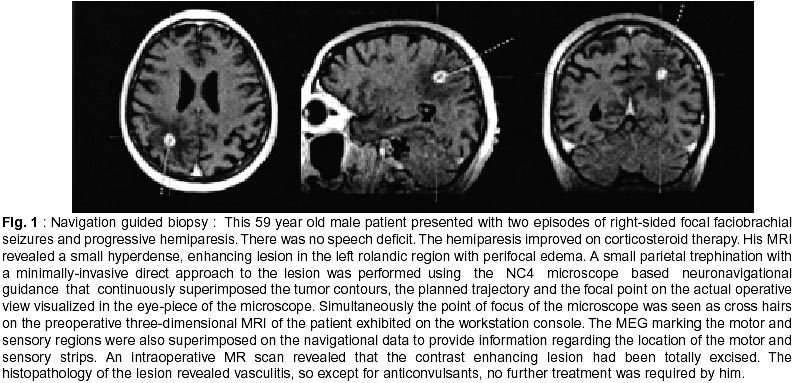
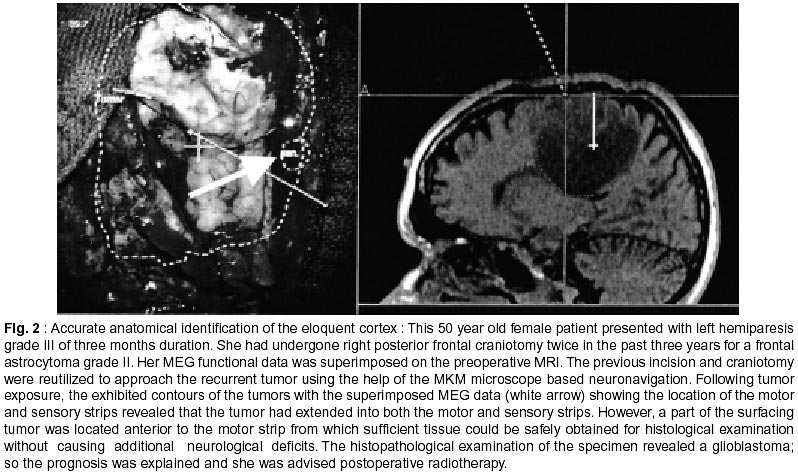
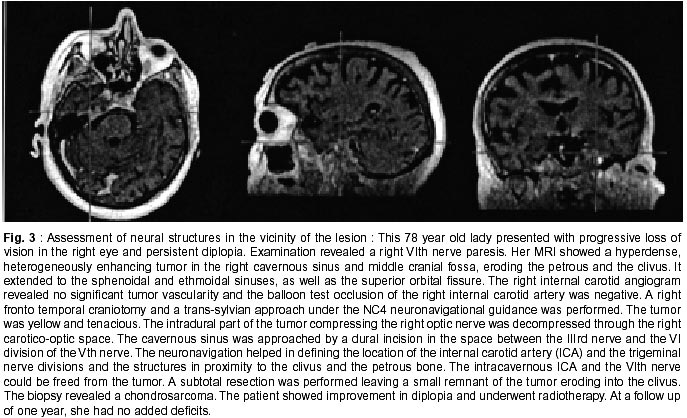
Rae Bareli Road, Lucknow - 226 014, India. Accepted for publication : 2nd April, 2002 Code Number: ni02076 Summary Neuronavigation provides intraoperative orientation to the surgeon, helps in planning a precise surgical approach to the targetted lesion and defines the surrounding neurovascular structures. Incorporation of the functional data provided by functional MRI and magnetoencephalography (MEG) with neuronavigation helps to avoid the eloquent areas of the brain during surgery. An intraoperative MRI enables radical resection of the lesions, the possibility of immediate control for tumor remnants and updates of neuronavigation with intraoperative images to compensate for brain shift. In this study, the experience of 432 patients undergoing neuronavigation assisted neurosurgical interventions using either the pointer-based or microscope-based navigational systems at the University of Erlangen-Nuremberg, Germany is presented. The procedures included stereotactic biopsy (n=53), stereotactic cyst puncture/ventricular drainage (n=15), eloquent cortex/tumor localization to facilitate tumor resection, assessment of neurovascular structures in the vicinity of tumors of the sellar-suprasellar regions, skull base, posterior fossa and ventricular region (n=252), and, surgery for epilepsy (n=9). Functional brain mapping using fMRI and MEG and their integration with neuronavigation was carried out in 24 and 128 patients respectively. The simultaneous use of intraoperative MRI to look for the remaining tumor was done in 159 patients and the update of navigational data was carried out in 17 patients. The mean system accuracy obtained by using both the fiducial registration as well as anatomical landmark-surface fitting computer algorithm was 1.81 mm. This study reviews the relative merits and demerits of the pointer and microscope based navigational systems and also highlights the role of functional brain mapping and intraoperative MRI, when integrated with neuronavigation, in the surgical decision-making to offer the chances of more radical resections with minimal morbidity. Key words : Frameless stereotaxy, Intraoperative MRI, Functional neuronavigation, Magnetoencephalography, Glioma surgery. Introduction Image-guided neuronavigation utilizes the principle of stereotaxis. The brain is considered as a geometric volume which can be divided by three imaginary intersecting spatial planes, orthogonal to each other (horizontal, frontal and sagittal) based on the Cartesian coordinate system. Any point within the brain can be specified by measuring its distance along these three intersecting planes. Neuronavigation provides a precise surgical guidance by referencing this coordinate system of the brain with a parallel coordinate system of the three-dimensional image data of the patient that is displayed on the console of the computer-workstation so that the medical images become point-to-point maps of the corresponding actual locations within the brain.1,2 The integration of functional imaging modalities, in particular, the magnetoencephalography (MEG), functional magnetic resonance imaging (fMRI) and positron emission tomography (PET) with neuronavigation has permitted surgery in the vicinity of eloquent brain areas with minimum morbidity.3-5 The spatial accuracy of the modern neuronavigation system is further enhanced by the use of intraoperative MRI that provides real-time images to document the residual lesion and to assess for brain shift during surgery.6-12 This article reviews the role and the current applications of neuronavigation and describes our experience using three different neuronavigational devices. Material and Methods In the period between June 1995 and May 2001, a total of 432 patients underwent neurosurgical interventions using the assistance of intraoperative neuronavigational systems at the University of Erlangen, Nuremberg, Germany. The patient's ages ranged from 2 to 85 years (mean : 44.30 years) and there were 246 male and 186 female patients. The intraoperative image guidance was achieved either by a pointer based system using the Stealth Station (Medtronic USA) or by a microscope-based system using the NC-4 or the multiple coordinate manipulator (MKM) neuronavigational microscopes (Zeiss, Oberkochen, Germany) and the standard STP 4.0 navigational software (Zeiss) (Table I). One day before surgery, 7 to 10 skin fiducial markers were attached to the patient's head and a three-dimensional fast low-angle shot sequence (TE, 7.0ms; TR 16.1 ms; flip angle, 30°; slab 168mm, 112 slices; FOV 250 mm, matrix 256 x 256) was taken with a 0.2 T Magnetom open MRI scanner (Siemens AG, Erlangen, Germany). This three dimensional data was transferred via fast-ethernet using the digital imaging and communications in medicine protocol (DICOM3) to the surgical navigation computer workstation. The determination of a specific point in the image space of this workstation that is corresponding to its actual location during surgery requires registration of the system to the fiducials on the patient.13 At surgery, once the patient's head was fixed to the Mayfield head holder, the process of registration was carried out by pointing the hand-held stereotactic pointing device of the Stealth Station system at each fiducial marker or by directly focussing each fiducial marker with the navigational microscope. The navigation accuracy was ascertained by inspection of anatomical landmarks. There are differences in the working methodology of the three navigational systems used in the present series. The Stealth Station consists of a mounted array of three charge-coupled device (CCD) cameras, a mobile computer workstation with a high resolution monitor, a dynamic reference frame (DRF) attached to the Mayfield head holder and a free handheld stereotactic pointing device. The DRF and the pointing device are mounted with infrared light emitting diodes (LED). The camera array measures the location of these LED that are processed to three dimensional coordinates in the computer workstation. Thus, a direct line of sight between the LED and the cameras must be maintained. The DRF mounted on the the intraoperative head stabilization device acts as a reference for the patient position so that if the operating table is moved, the navigation system defines the patient's new location and the navigation can continue. The LED on the pointing device calculates the location of its tip and displays the location as a cross-hair on the three-dimensional image data set on the workstation console.2,14,15 In the NC4 microscope, the infrared emitting LED are mounted on the microscope itself. These can be captured by the overhead array of CCD cameras and the position of the microscope relative to the patient can be defined after the standard patient-to-image registration. The focal point of the microscope during actual surgery is used in place of navigation with a pointer and is displayed on a corresponding point of the preoperative image data exhibited on the monitor of the workstation . In the MKM neuronavigational system, the microscope is mounted on a high precision robotic arm integrated into a neuronavigation system that continuously references and updates the microscope position relative to the patient once the standard patient-image registration procedure has been performed. Thus, an overhead CCD camera to detect the position of the microscope is not required. In both these microscope based systems, the navigation data visible on the workstation console can also be displayed into the eyepiece of the microscope. It is therefore possible to visualize within the microscopic image both the superimposed contours of the targetted lesion and the predefined surgical approach as well as the position of the focal point of the microscope.14,16,17 Integration with functional data for cortical localization : Morbidity during neurosurgery in proximity to the eloquent areas can be considerably reduced by functional brain mapping and its combination with neuronavigation (Table II). The functional brain mapping was performed by two techniques at our centre : Functional MRI was carried out by a 1.5 T MR scanner (Magnetom Symphony; Siemens AG, Erlangen, Germany) to rapidly acquire 16 contiguous T2* weighted MR slices (TE, 62ms; TR, 114ms; flip angle, 90°; slice thickness, 3mm; FOV, 200mm; matrix, 64 x 64; interpolated 128 x 128), parallel to the anterior-posterior commissure plane, ranging from the parietal operculum to the vertex by utilizing the technique of echoplanar imaging.18-20 When motor and sensory activity were carried out, this T2 weighted MR sequence detected as hyperintense signals, the significant increase in oxyhemoglobin concentration with a relative decrease in the paramagnetic deoxyhaemoglobin concentration in the capillaries and venous blood reflecting the increase in the local blood volume far in excess of the metabolic demands as well as the utilization of anerobic metabolism by the transient neuronal activity in the relevant region of the brain (the blood oxygen level dependent [BOLD] technique).21-23 The echoplanar imaging rapidly acquired successive images of the entire volume of interest of the brain with a high resolution (image acquisition times of 70 to 100 milliseconds and isotropic 3 mm resolution.4,8,20, 24 The motor evoked activity (MEA) was performed by clenching of the hand contralateral to the side of the lesion at the rate of one per second; and, the sensory evoked activity (SEA), by administering tactile stimuli at intervals of 800 msec to the index finger contralateral to the lesion by means of a tactile stimulater in the form of a finger clip. 10 fMRI volumes each were recorded during three activation and three rest periods respectively. In identical axial MRI slices using T1 weighted spin echo sequences (TE,15ms; TR, 450msec; flip angle, 90°; slice thickness, 3mm; FOV, 200mm; matrix, 256 X 256), anatomical images were also acquired.8 Correlating the functional and anatomical data, functional activation maps were calculated, utilizing the methods suggested by Bandettini et al,25 and Xiong et al,26 using the AFNI software.27 The draining veins of the activated cortex carrying deoxygenated blood may give an overestimation of the area representing the functional cortex so the anatomical and the functional images were correlated with respect to the draining veins and suitable corrections performed.21,24 The method for the localisation of the speech areas was described elesewhere.19 Magnetoencephalography (MEG) : The Magnes II biomagnetometer (Biomagnetic Technologies Inc, San Diego, Ca, USA) with 2 x 37 multichannels was used for the MEG recording in a magnetic-shielded room. This device contains highly sensitive superconductive quantum interference devices (SQUID) that detect from the scalp, neuronal neuromagnetic signals reflecting the intracellular current flow in the apical dendrites of pyramidal cells oriented tangential to the scalp surface. It works on two simplifying assumptions : a) that the head is a sphere of uniform conductivity; and, b) that the detected electromagnetic field is generated by only one point-source current dipole.3,28-30 Initially the patient's head was scanned relative to the MEG sensors with an electromagnetic threedimensional digitizer. Then, motor activation was perfomed by brisk flexion movement of the index finger contralateral to the lesion every 3 to 5 seconds. The sensory activation was identical to that used in functional MRI. 200 stimuli of SEA, and 100 stimuli of MEA were acquired. A simultaneous EMG recording of flexor digitorum indices muscle was also done and a single movement of the index finger triggered off a signal of this EMG recording. The MEA were measured 2 seconds before to 1 second after the EMG onset. Motor artifacts were avoided by stabilizing the patient's arm and placing the head in an vacuum cushion. The motor and sensory events produced fluctuations in the local magnetic field that were detected across the sensory array of the MEG and could be described by an isofield contour map. The somatosensory neuromagnetic waves representing the primary sensory cortex peaked from 20 to 100 msec31 and the motor evoked waves representing the motor areas showed marked activity at a latency of 100 msec after the EMG onset.32 Mathematical models inferred the location of the neurons responsible for the recorded magnetic pattern. These MEG determined source locations were plotted on spatially aligned MRI via transformation of the MR and MEG coordinate system by a contour fit program, fitting the digitally scanned head shape including the MEG dipole source to the patient's MRI data.33 This three dimensional FMRI or the MEG data was then transferred via fast ethernet to the neuronavigation microscope for functional neuronavigation during surgery.3 In the initial cases, for confirmation of the displayed functional data, intraoperative phase reversal of somatosensory evoked potential was also measured with strip electrodes by stimulating the median nerve at the wrist with 300 repeated, 0.1 msec constant current pulses delivered at a frequency of 5.1 Hz and a current strength of 10 to 20 mA4 (Table II). Integration with an intraoperative MRI : Since December 1995, a twin Operating room (OR) concept has been implemented in our department.6-8,35-37 The open MRI system has been located in the radiofrequency shielded OR which also includes an MRI compatible anesthesia monitoring system. The MKM microscope has been located in the adjacent conventional OR. The surgical procedures have been carried out after the tumor borders and functional measurements from preoperative images have been superimposed on the viewing field of this navigational microscope. For conducting the intraoperative MRI, the patient lying on an air-cushioned OR table was shifted to the radiofrequency shielded OR ( a distance of approximately 5 m from the conventional OR room) for MRI.8,12,37 20 ml of gadolinium diethylene triamine penta-acetic acid was administered intravenously if the preoperative MRI showed tumor enhancement. In low grade astrocytomas, apart from the three- dimensional flash gradient echo sequence, a T2W sequence (slice thickness 3mm; TR 6000ms; TE 117 ms; FOV 230mm) was also performed. When the intraoperative MRI revealed tumor remnants, then further resection was possible during the same operation (so-called second look) 8. In the cases where full resection was not possible due to the proximity of the lesion to eloquent anatomical locations, the intraoperative MRI still enabled immediate additional therapy planning rather than delaying the decision while waiting 2 to 3 months for repeating an artifact-free postoperative MRI. This intraoperative transportation of the patients in the twin OR has been necessary in order to obviate the need for MR compatible instrumentation; and, for free patient access as well as for full availability of the neuronavigation systems incorporating the functional data. However, the transportation led to loss of neuronavigation registration. When intraperative registration of the new imaging data to update neuronavigation (in order to navigate to the residual tumor and to compensate for brain shift) was required, 5 bony fiducials were placed around the craniotomy opening; the intraoperative three-dimensional MRI data was transferred via ethernet to the MKM navigation microscope; the bony fiducials were identified in the intraoperative images; the remaining tumor was segmented and an approach was planned. The patient-image registration was performed with these markers to complete the updating of the navigation with the intraoperative images. The calculated technical accuracy (less than 2mm) and landmark checks maintained the accuracy by the upgraded navigation. This neuronavigation updating added 15 minutes to the operating time. However, in cases where easily located tumor remnants were revealed by the intraoperative MRI, the surgery was continued without updated navigation (Table III). The procedure of intaoperative shifting of patients for intraoperative MRI was cumbersome. To circumvent this, since May 1999, an NC4 navigation microscope, with a camera for tracking its movements, has been placed in the radiofrequency shielded OR at a distance of 2 to 2.3m from the centre of the MR magnet (corresponding to a magnetic field strength of 10 to 5 G) while its work-station has been placed outside the OR so that its functioning would not be affected by the magnetic field. The patient has been operated on the MR table 1.5 to 1.7m from the magnet (corresponding to a magnetic field strength of 30 to 15 G). At this distance from the center of the 0.2 T magnet, the registration accuracy of the neuronavigation remained within acceptable limits (less than 2mm), there was no distortion of the contour of the microscope headsup display and there was no magnetic pull in the direction of the magnet when the microscope was unlocked. Thus it was possible to combine navigationaided neurosurgery with intraoperative MRI without the time consuming and cumbersome intraoperative transfer of the patient from one OR to the other and without the need for special MR compatible surgical instrumentation.8 However, once the position of patient was shifted to the centre of the magnet for an intraoperative MR, a neuronavigation update with new intraoperative image data was again required as the original patient-image registration was lost. Moreover, it was not possible to change the position of the patient's head during surgery once he/she has been placed on the MR table and the head fixed on an MR compatible ceramic head holder.6-8,37-39 The pre- and intraoperative three dimensional imaging data was also compared for brain shift7 by performing a rigid registration of the two using 6 to 12 anatomical landmarks or fiducial markers. A continuous transition of skin surface in the pre- and intraoperative images in all displayed planes and an overlap of the location of the basilar artery were documented to ensure perfect mapping of the pre- and intraoperative images. The maximal displacement of the cortical surface, the deep tumor margins, the midline and the mean value of shift of atleast 6 different landmarks of the ventricular system were measured. In addition, the patient's position during surgery and the tumor volume were also noted.7,8,11,39 Clinical applications and results The clinical application and the results are summarised in Table IV. Illustrative cases are depicted in Fig. 1, Fig, 2, and Fig. 3. Discussion Neuronavigation : In the present series, neuronavigation was useful in providing orientation to the surgeon with sufficient application accuracy. It facilitated a precise planning of the craniotomy and of the surgical vector to the targetted small, subcortical lesions; in astrocytomas, it helped to define the tumor margins and the limits of resection,13 in skull base lesions, it was useful in localizing encased and displaced vascular structures, the tumor extension into various brain crevices and the position of osseous landmarks.40 Golfinos and colleagues1 have also elucidated its role in epilepsy surgery in predicting the length of the corpus callosum division in corpus callosectomy, in judging the posterior margin of the anterior temporal resection and in localizing the hippocampus; and, in endoscopic surgery, where an orientation within the ventricular system was provided. There are, however, certain technical drawbacks that make its usefulness suboptimal. The probe of the stealth station is bulky restricting its manipulation under the microscope and its introduction into narrow operative fields e.g. the cerebellopontine angle or the petrous bone. The view of the surgeon must change from the microscope to the workstation console, while localizing an anatomical structure with its probe which may inadvertently cause neurological trauma. The requirement of an uninterrupted line of sight between the LED and the camera array required in the stealth station and the NC4 neuronavigational microscope hampers movement in the OR. The robotic arm of the MKM microscope is too slow to permit frequent changes of the angle of view especially for skull base procedures. In both the microscope based systems, the information display projected into the microscope eye-piece is twodimensional and therefore user-unfriendly and once the patient-to-image registration is achieved, the patient's head cannot be moved to gain a more optimal operating position as that would lead to loss of registration.40,41 Implementation of a dynamic patient tracking solved that problem. The frameless neuronavigational systems other than the three used in the present series include: a) a digitizing mechanical arm with potentiometers in its six joints that calculate the position of the arm or probe tip from the angle of the various joints,1,2,14,41-51 though simple to use, it is bulky, b) the ultrasound based systems, where the ultrasound pulse emitters mounted on the robe are detected by multiple microphones and the delay between the production and reception of the pulse is used to determine the position of the localizing device. The image guidance in this method directly depends upon the distance between the emitter and the transmitter and the maintenance of a direct line of sound between the two. Moreover, changes in the speed of sound by temperature, humidity, air currants, extraneous echoes, radiofrequency emissions and sonic reflectors in the OR may affect its accuracy, and c) the electromagnetic systems,52,53 where the localizing device has low frequency electromagnetic field transmitters which generate an electromagnetic field that is detected by sensors to provide updated information regarding its position. The usage of the electromagnetic systems is not widespread. Registration : An accurate and reliable neuronavigation requires a low system error and a high rate of congruence between the patient's preoperative three dimensional images and the surgical anatomy. This patient-to-image registration can be achieved either by correlating fiducials on the skin or bone or by matching external rigid landmarks.1 In order to enhance the precision of registration in our patients, a surface-matching of the contours of the surface of head to the contours of the head visible on MRI was also performed. During surgery, a system-check was obtained by localizing deep bony landmarks. The overall accuracy of the system was ascertained by comparing the fiducial coordinates on the dispalyed images to actual coordinates obtained from physical registration of the patient's head and noting the amount of deviation from each registered fiducial. Zinreich et al, defined the limits of the best accuracy (an average of 1-2mm) that can be expected in vivo, by testing the viewing wand system on a plastic model of the skull.54 Golfinos et al, achieved an accuracy of 2mm in 82% of their patients using CT images and 92% using MR images and felt that the more acurate registration with MR than CT was because of greater familiarity with MRI reconstruction in multiple planes.1 In the present series, the mean system accuracy obtained by using both the fiducial registration as well as anatomical landmark-surface fitting computer algorithm was 1.81 mm, which is comparable to the accuracy reported in the other published series that ranges from 1.6mm to 3mm.1,43,45,55 In the case of lesions of the posterior fossa, however, the error in accuracy was much higher the usefulness of neuronavigation in this region of important neurovascular structures that exist in close proximity. In lesions in and around the petrous bone, a higher application accuracy than the 2 to 3mm precision that is routinely available is required due to the close proximity of important anatomical structures. Moreover, anatomical features and externally based fiducials, except the non-rigid outer ear, are not available for providing spatial inputs to the patient image registration and therefore bony landmarks such as the emissary foramina, footplate of stapes, facial nerve genu, round window, ampulla of lateral or superior semicircular canals or the canal of internal carotid artery have to be used.2,14 The accuracy of the system is compromised by many factors. The slice thickness of the scanned image determines its voxel resolution and therefore its accuracy of registration. Interpolation of voxel intensities during reformatting of images further enhances the registration error.] Patient motion; artifacts in the CT or MR scans; change of position of the fiducials or shifting of the skin; faulty placement of probe on the exact location of CT and MR images; and, errors in the contouring of tumor volume may all compromise registration.1,2 As the actual surgical position is related to the images acquired preoperatively, a progressive error in registration is observed during intraoperative navigation due to the brain shift7,11,39 which depends on the patient position, brain edema, bleeding, cerebrospinal fluid volume change, tumor removal, cerebral blood volume, use of mechanical ventilators or diuretics or retraction during surgery.2 Dorward et al, quantified brain shifts during open cranial surgery to assess the impact of postimaging brain distortion on neuronavigation and reported a mean shift of 4.6mm of the cortical surface after the dural opening and 6.7 mm at completion of tumor resection. The shift at the deep tumor margins in cases of convexity meningiomas was significantly more than gliomas while skull base lesions demonstrated little brain shift.39 In this study, an intraoperative MRI was used to calculate the brain shift and to update the neuronavigational system to eliminate the inaccuracies occurring in the system due to this phenomenon. Following tumor resection, the brain surface sank 7 mm below the dural level in 60 to 70% of patients in whom it was assessed. This surface brain shift may interfere with the identification of eloquent cortical areas during functional neuronavigation.7 In the present series, in cases in whom the deep tumor magin shift was measured, it exceeded 3 mm in nearly 70% of the cases. The deep tumor margin-shift does not interfere with the accuracy of neuronavigation during surgery for the skull base lesions. In these cases, therefore, an assessment of shifts of important neurovascular structures surrounding the tumors is more useful than the measurement of brain surface shifts.7 Also serial intraoperative MRI provides an accurate basis for the computational analyses of brain deformations that may be used for intraoperative guidance during neuronavigation.11 Intraoperative three-dimensional ultrasonography,57 various mathematical models and modification of the preoperative imaging data to match the real time deformed brain have also been proposed to evaluate and compensate for the inaccuracies that occur in neuronavigation due to brain shift during surgery.7 Functional imaging: Definition of the eloquent areas by the fMRI and MEG and the incorporation of this information in the image data being used for neuronavigation helped to plan a trajectory that avoided these regions and minimized the morbidity of the procedure. The advantages of fMRI are the wide availability of the MRI facilities, absence of ionizing radiation and the provision of both the anatomical and functional data utilizing the same imaging modality by image fusion with a three-dimensional MRI. However, the image acquisition time is long and the haemodynamic changes that the FMRI detects, take several seconds to develop and therefore do not reflect the real time brain activation no matter how fast the image acquisition time is. Moreover, the deoxygenated blood in the cortical veins may cause errors in the sensory-motor localization.3,22,23,58 In the MEG, the scalp recordings reflect the instantaneous changes in the intracranial electromagnetic field evoked by the peripheral motor and sensory stimuli.3 It, however, requires image fusion with structural MRI to give a precise location of the lesion and the technology is restricted to a few centres only. The mean difference in the functional localization using the fMRI versus MEG data in various series has ranged from 10 mm59 to 16 mm58 and was 14 mm in the present series. However, for identification of the central sulcus there was a fairly good agreement between the two.3-58,60A good match was demonstrated between the cortical sensorimotor localization achieved by the fMRI/MEG as well as by the conventional median nerve SSEP in the 66 cases in whom both were done (Table II). Intraoperative MRI : In our series, the navigation microscope with integrated neuronavigational and functional data (from fMRI and MEG) was used to perform surgery at the fringe field of the 0.2 T magnet of the Magnetom Open utilizing standard instrumentation.4,6,7,35,37 Thus, the lesion was targetted using neuronavigation; the functional data allowed preservation of eloquent brain areas3 and, intraoperative MRI enabled radical resection of lesions and the possiblity of the second look for tumor remnants.8,35-37 Neuronavigation could be further updated with intraoperative images to compensate for brain shift in case the second look procedure required navigation.7,11 The limitations with repect to the constraints of space for the surgeons and nurses as well as the mandatory MRI compatibility of the surgical instruments imposed by the double-doughnut design of the intraoperative MRI (General Electric Medical Systems, Milwaukee)9-11 have been overcome by the open magnetom MRI used in this series.7,8,11,35,37 Moreover, the integration of the microscope based neuronavigation system that was done in the Magnetom Open MRI system in this study is not possible with the double-doughnut MRI because the microscope must be placed very near the centre of the magnetic field in the latter system. Enhancing the capability of the intraoperative MRI would enable its utilization for fMRI, spectroscopy, diffusion, perfusion and angiography and the integration of these imaging modalities into neuronavigation .6 However, the interpretation of the intraoperative MRI scan may be affected by diffuse enhancement at the resection border due to the disruption of the bloodbrain barrier, surgicel placed at the resection site or by the surrounding edema. In pituitary adenomas, collected blood may interfere with the identification of the residual tumor.7 Conclusion This study reviews a few of the applications and frontiers in the field of neuronavigation. Progressive advances in technology will improve the cost-benefit ratio and the user-friendliness of the system and in the near future it may help to realize the aim of complete cytoreductive surgery with minimal morbidity. However, at the present state of kowledge, the benefits of neuronavigation only compliment the experience and knowledge of neuroanatomy of the surgeon and cannot act as a substitute for it. Acknowledgement This work had been supported by a UICC International Cancer Technology Transfer Fellowship and Funds for Scientific and Educational activities of the University of Erlangen-Nurembeg. Germany. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02076t2.jpg] [ni02076f3.jpg] [ni02076t4.jpg] [ni02076t3.jpg] [ni02076t1.jpg] [ni02076f2.jpg] [ni02076f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}