 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 262-266 Neurophysiological Changes in Japanese Encephalitis J. Kalita, U.K. Misra Department of Neurology,
Sanjay Gandhi Postgraduate Institute of Medical Sciences,
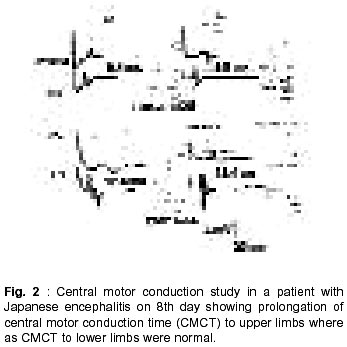
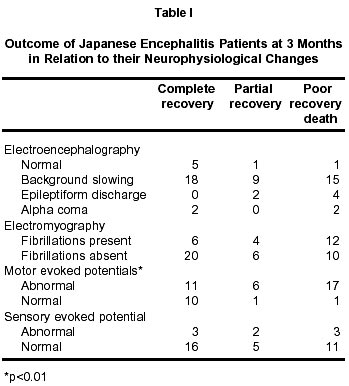
Lucknow- 226 014, India. Accepted for publication : 20th July, 2002. Code Number: ni02078 Summary Japanese encephalitis (JE) is an encephalomyelitis involving cortex, subcortex, brainstem and spinal cord. There is paucity of studies on the neurophysiological evaluation in JE. This study aims at comprehensive evaluation of EEG, sensory and motor evoked potentials, nerve conduction and electromyography; and correlate these with clinical findings. Sixty five patients with JE diagnosed on the basis of clinical, radiological and virological criteria were subjected to a detailed clinical evaluation during the acute stage of illness. Cranial CT scan or MRI was carried out in all the patients. All the patients underwent 10 or 18 channel EEG, motor and sensory evoked potentials to both upper and lower limbs bilaterally as well as peroneal and sural nerve conductions and concentric needle EMG. Outcome, was defined at the end of 3 months into poor, partial and complete recovery. The patient's age ranged between 2-65 years. There were 40 males and 25 female patients. Fifteen patients were less than 12 years of age. History of seizure was present in 31 patients. Quadriplegia was seen in 39 and hemiplegia in 8 patients. Muscle wasting was present in 16 patients and tendon reflexes were reduced in 12 and of mixed pattern in 14 patients. Cranial MRI revealed thalamic lesion in 38, basal ganglia in 21, substantia nigra in 30, pons in 5, cerebellum in 3 and cerebral cortex in 7 patients out of 57 patients. EEG revealed nonspecific theta to delta slowing in 45, alpha pattern coma in 5 and epileptiform discharges in 8 patients. EMG revealed fibrillations in 23 patients. Motor evoked potentials were abnormal in 34 out of 46 patients and revealed patchy and focal abnormalities comprising of unrecordable, prolonged and normal pattern. Somatosensory evoked potentials were abnormal in 8 patients only. At 3 month, 26 patients had complete, 13 partial and 15 had poor outcome. Eight patients died in acute stage and 3 were lost to followup. MEP correlated with weakness and 3 month outcome whereas EEG, SEP and EMG did not have any correlation. MEP changes were more frequent in JE and had prognostic significance. Key words : Encephalitis, Japanese, EEG, MEP, SEP, EMG, MRI, Outcome. Introduction Japanese encephalitis is the commonest human endemic encephalitis, mainly restricted to south east Asia. It is a disease seen more commonly in rural areas and has been linked to paddy cultivation, pig farming and mosquito breeding. A comprehensive account of neurophysiological changes is not available because of these epidemiological characteristics and paucity of investigative facilities in these areas. However, isolated studies on EEG, evoked potential and EMG have been reported.1-3 JE is an encephalomyelitis affecting brain, spinal cord and anterior horn cells. The involvement of these structures can be evaluated by EEG, evoked potential and EMG studies.4 In this communication, we report EEG, evoked potential and EMG changes in 65 patients with JE and correlate these changes with clinical findings. Material and Methods Sixty five patients with JE during acute stage of illness were included in this study who were managed by us during 1992 to 1999. The diagnosis of JE was based on the following criterias. Essential criteria : Patients presenting with acute encephalitic syndrome, characterized by fever and altered sensorium in whom malaria and septic meningitis have been excluded. Supportive criteria : a) Patients coming from known JE endemic area, b) fourfold rise of IgG antibodies against JE virus by hemagglutination inhibition test. c) Thalamic involvement on CT or MRI scan. Patients fulfilling the essential and two of the three supportive criteria were included in the study.1 A detailed neurological evaluation was carried out in all the patients. The level of consciousness was assessed by Glasgow coma scale. Presence of seizures, behavioral abnormality, focal weakness, wasting and reflex changes were noted in all the patients. Sensations of pinprick, joint position and vibration were tested in the patients who could cooperate for these tests. Cranial CT scan was carried out using a third generation CT scanner. 10 mm axial sections were obtained. Cranial MRI was carried out on a 2T scanner operating at 1.5 T (Magnetome SP, Siemens Germany). T1, PD and T2 weighted spin echo sequences were obtained. The neurophysiological investigations included electroencephalography, peroneal and sural nerve conduction, concentric needle electromyography and motor and somatosensory evoked potentials studies. All these tests were carried out during acute stage (4-15 days) except EMG which was carried out after 2 weeks. EEG was recorded for 30 minutes. Median somatosensory evoked potentials (SEPs) were analyzed by the latency of N9, N20 and interpeak latency of N9, N20. For tibial SEPs laten cies of N21, P40 and N21 - N40 were measured.5-6 The upper limit of normal was defined by mean+2.5 SD of controls. The upper limit of CMCT-ADM (mean+SD) was 8.1 (5.1+1.2) ms, CMCT - TA 16.1 (12.1+1.6) ms, median N9 - N20 conduction time was 11.3 (8.3+1.2) ms and tibial N21-N40 conduction time was 27.1 (20.1+1.2) ms. The relationship between various clinical, radiological and neurophysiological parameters was evaluated employing X2 test. For evaluating the relationship of seizure, weakness and lower motor neuron signs EEG was catergorized into with epileptiform discharge or without, CMCT into normal and abnormal (unrecordable or prolonged) and EMG into presence of denervation or without these changes respectively. For evaluating the relationship of various EEG changes and radiological changes the latter were classified into normal, presence of cortical lesions and others. The outcome of the patients was defined at the end of 3 months into poor, partial and complete. The poor recovery was defined as bed ridden states, partial as dependence for activities of daily living and complete as independent for activities of daily living.4 Death was included in poor recovery group for statistical analysis. The relationship of outcome (poor, partial and complete) was also correlated with EEG (normal, slowing, alpha coma and epileptiform discharge), EMG (denervation or not), CMCT (abnormal or normal) and SEP (normal and abnormal) employing X2 test. Results Sixty five patients with JE, with age range of 2 and 65 years, were included in this study. There were 40 male and 25 female patients. Fifteen patients were 12 years of age. Signs of meningeal irritation were present in 11 and history of seizures in 31 patients. Decerebration or decortication was present in 33 patients and behavioral abnormalities in 11 patients. Glasgow coma scale score ranged between 3 and 15 (mean 7.4). Focal weakness in the form of quadriplegia was present in 39 and hemiplegia in 8 patients. Cranial nerve palsy was noted in 7 patients; one patient had complete ophthalmoplegia, two had facial palsy and abducence palsy. Bulbar weakness and optic atrophy was noted in one each. Muscle wasting was present in 16 patients which was generalized in 5 and focal in the remaining. Muscle tone was decreased in 15, normal in 11 and mixed type in 3 and increased in the remaining patients. Tendon reflexes were exaggerated in 15, reduced in 12, normal in 14 patients and mixed pattern was present in the remaining 24 patients. Sensations could not be evaluated in the acute stage however, later when patients could cooperate, sensations were normal in all. CT scan was done in 60 patients. Thalamic involvement was noted in 17 patients which was bilateral in all except two. Basal ganglia hypodensity was present in 3 and mid brain and cerebellum in one case each. One patient had evidence of associated neurocysticercosis. Cranial MRI was done in 57 patients which revealed of thalam involvement in 38 patients, basal ganglia in 21, substantia nigra in 30, pons in 5, cerebellum in 3 and cerebral cortex in 7 patients. Neurophysiological findings : EEG revealed nonspecific slowing of background activity mainly in delta to theta range in 52 patients (Fig. 1). Alpha pattern coma was seen in 5 cases. Remaining 8 patients had normal EEG. There was no voltage and frequency asymmetry. Spike and wave discharges were present in 8 patients. The patients with alpha pattern coma had deep coma. Their EEG activity did not change on giving pinprick and loud sound. Sural nerve conductions were normal in all the patients. Peroneal conductions were unrecordable in 5 patients. There was marginal slowing of conduction velocity in 3 and in the remaining patients, conduction velocity was normal although compound muscle action potential was reduced in 4 patients. Concentric needle EMG after two weeks of ictus revealed fibrillations in 23 patients. The fibrillations were present in all the four limbs in 5 patients, whereas in the remaining 18 patients fibrillations were present in the weak or wasted muscles with corresponding areflexia. The motor unit potentials were polyphasic and long duration with poor recruitment. Evoked potential studies were carried out in patients of > 12 year of age. Motor evoked potentials were carried out in 46 patients. Central motor conduction time was abnormal in 34 patients. CMCT-ADM was unrecordable in 8 patients (15 sides) and prolonged in 32 patients (36 sides). In 15 patients, CMCT- ADM was prolonged on one side only and it was normal on the other side (Fig. 2). CMCT-TA was unrecordable in 7 patients (13 sides), prolonged in 11 patients (20 sides) and was normal in 28 patients. Somatosensory evoked potentials were carried out in 43 patients and were abnormal in 8 patients only. Median SEP was abnormal in 5 patients out of 38; unrecordable in 2 (4 sides) and prolonged in 3 patients (4 sides). Tibial SEP was abnormal in 5 out of 42 patients. It was unrecordable in 3 patients (5 sides) and prolonged in 2 patients (2 sides). EEG changes did not correlate with the history of seizures (X2=0.28, df=1, NS). Interictal EEG revealed epileptiform discharges in 4 out of 31 patients with seizures whereas 3 out of 34 patients without seizures also had epileptiform discharges. Radiological changes were not correlated with various pattern of EEG abnormality (X2=1.98, df=6, NS). Patients with normal CT and/or MRI also had slowing (7), epileptiform discharge (2) and alpha coma (1). Thalamus, basal ganglia and brainstem lesions were also associated with slowing (33), epileptiform discharges (5), alpha coma (3) and even normal EEG (6). EMG correlated with the evidences of lower motor signs (X2=28.03, df=1, p<0.01). Out of 27 patients with lower motor neuron signs, 20 had fibrillations and sharp waves or both on EMG and 3 out of 35 patients without lower motor signs also had EMG evidences of denervation. Motor evoked potential correlated with weakness (X2=11.8, df=1, p<0.01). MEP was abnormal in 29 out of 33 patients with weakness whereas only 5 out of 13 patients without weakness had MEP abnormalities. At the end of 3 months, 26 patients had complete, 13 partial and 15 had poor outcome and 8 expired. Out come at 3 months did not correlate with EEG (X2=8.04, df=6, NS), EMG (X2=5.03, df=2, NS) and SEP abnormality (X2=0.55, df=1, NS) but did correlate with MEP changes (X2=9.49, df=2, p<0.01). The details are summarized in Table 1. Discussion In the present study, EEG was abnormal in 88%, MEP in 70%, EMG in 35% and SEP in 19% patients with JE. High frequency of EEG abnormality is consistent with widespread subcortical and cortical involvement in JE. The commonest EEG abnormality was delta to theta slowing. This was consistent with high frequency of thalamic involvement in our patients. Diffuse delta slowing is a characteristic of variety of comatose states regardless of the etiology.7 Delta activity occurs due to subcortical deep frontal supratentorial lesions and various metabolic encephalopathies.8,9 Thalamic lesion produces delta activity of varying degree and extent encompassing the whole ipsilateral hemisphere. Delta waves can be generated by the lesion of thalamus.1,4,10 The other EEG abnormality was lateralized epileptiform discharges in 8 patients, although it was associated with corresponding cortical involvement in one patient only. The epileptic discharges on EEG were not correlated with cortical lesion on CT or MRI scan. Absence of imaging changes does not exclude cortical dysfunction in encephalitis. Alpha pattern coma was present in 5 patients and is attributed to characteristic frontomesencephalic junctional abnormality, which is severe enough to produce coma but not enough to suppress thalamus which is responsible for generation of alpha waves.11 Although, history of seizures was present in 31 patients but epileptiform discharges were present in 8 patients only. The low frequency of epileptic discharge on EEG may be due to the first EEG recording in the hospital whereas the seizures occurred earlier either at home or primary medical care centre. The evoked potential changes were characterized by high frequency of motor evoked potential abnormalities which was associated with various permutation and combination of unrecordable, prolonged and normal recordings which were patchy and focal. In the cerebral cortex, the frontal cortex is most commonly affected in JE.12 The histopathological changes in JE include edema, congestion, focal hemorrhage of brain and meningitis. The CMCT abnormality could be attributed to the involvement of central motor pathways at cortical, subcortical or spinal cord level. Slowing of central motor conduction time is not only due to damage or demyelination or motor pathways but also because of desynchronization of descending volleys to the anterior horn cells.13 Paucity of sensory abnormality was evidenced by low frequency of SEP abnormality being present in 8 patients only. This is consistent with our earlier report where only one tibial SEP was unrecordable.4 As the patient regained consciousness, sensory abnormalities were not found clinically in any patient. Rarity of SEP abnormality in view of high frequency of thalamic nvolvement in JE is interesting and may be due to relative sparing of sensory pathways. Fibrillations on EMG were present in 35% patients which may be due to anterior horn cell involvement. Recently, polio like illness due to JE has been reported from Vietnam.14 We had also reported earlier a high frequency of anterior horn cell involvement based on clinical and EMG studies.2 Histopathological examination of spinal cord has revealed neuronolysis, neuronophagia with glial and leucocytic reaction simulating acute poliomyelitis.15 The neurophysiological studies although helped in documenting the specific neuronal system of pathway but could also have a role in predicting the outcome of JE. The motor evoked potential was significantly related to 3 month outcome whereas EEG, SEP and EMG were not. EEG changes were present almost in all the patients and did not discriminate between those with good or poor outcome. SEP change was too infrequent to be of prognostic significance. EMG although has not achieved statistical significance in the present study but was significant in our earlier study.16 In a multivariate analysis on prognostic predictors of JE, age, GCS score and reflex changes were the best predictors of 6 months outcome.16 Hyporeflexia during acute stage may be due to cerebral shock or extensive anterior horn cell damage or both. Anterior horn cell involvement in JE is usually overshadowed by pyramidal, extrapyramidal and cerebellar involvement and the outcome is determined by the overall neurological involvement rather than isolated involvement. From this study, it can be concluded that EEG changes are more frequent in JE, however, MEP abnormalities have more prognostic significance, which may be due to involvement of motor pathways at different levels. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02078f2.jpg] [ni02078f1.jpg] [ni02078t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}