 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
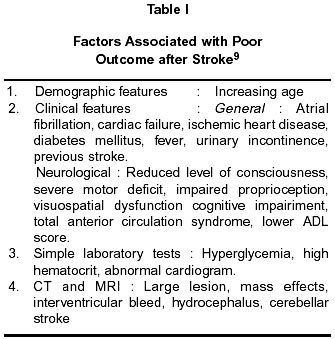
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 279-281 Predicting Mortality in Stroke A. Bhalla, O.P. Gupta, S.B. Gupta Department of Medicine,
MGIMS, Sevagram,
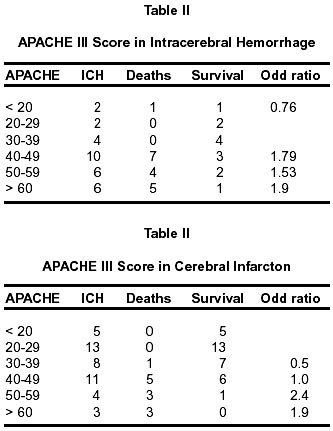
Wardha (MS)., Accepted for publication : 6th June, 2001. Code Number: ni02081 Summary Physicians are faced with the task of predicting the immediate and long term outcome in stroke patients. It is also important to efficiently and optimally utilize resources. We used APACHE III scoring system or predicting in hospital outcome in patients with stroke.We found it to be sensitive (>90%) and resonably specific (73%) in predicting short term, in-hospital mortality, in our study group. Key words : Stroke mortality, APACHE III scoring system. Introduction Stroke is the third major cause of death worldwide. The world wide incidence has been quoted as 2/1000 population/annum; about 4/1000 in people aged 45-84 years.1 In India the incidence of cerebrovascular disease was found to be 13/100,000 population/year in a study conducted at Vellore in 1969-71 and 33/100,000/ year in study conducted at Rohtak. A WHO study, in 1990 quoted incidence of mortality due to stroke in India to be 73/100,000 per year.2 The survival, recovery and ultimate outcome in stroke patients depends on various variables, out of which important ones are demographic, underlying medical disorders related, lesion related and specific therapy related (Table I). Physicians are faced with the task of predicting the immediate and long term outcome in variety of emergency situations but it is most difficult to do so in stroke patients. Aim of this study was to evaluate APACHE III scoring system as a method of prediction of mortality in stroke patients. Material and Methods This study was carried out at 12 bedded medical ICU at Mahatma Gandhi Institute of Medical Sciences, Sevagram over a period of 12 months. All the patients with stroke admitted to medical ICU were studied. These patients were evaluated clinically and CT scans were performed to confirm the diagnosis.APACHE III scoring system was used to calculate the score and this was correlated with the immediate in-hospital outcome of these patients.3 The sensitivity and specificity of this score was calculated at a cut off point of 40. Results Seventy four patients were admitted with diagnosis of stroke in one year. 30 patients had intra cerebral hemorrhage (40.5%) and 44 had infarction (59.5%). Seventeen patients out of 30 in the hemorrhagic group (56.6%) and 10 out of 44 (22.7%) in the infarctions group died. The overall mortality observed was 34% in all the patients (27/ 74 patients). The sensitivity and specificity of APACHE III scoring system in predicting mortality was 94.12% and 53.85% respectively, in patients with hemorrhage (Table II). 90% and 73.53% respectively for ischemic stroke when a cut off point of 40 was taken (Table III). It was also observed that the likelihood of mortality increased as the score increased. Discussion Acute stroke is a heterogeneous condition with respect to prognosis. At present it is impossible to predict outcome in an individual with greater accuracy.1 In acute stroke the chances of survival depend on various factors like neurological damage, systemic dysfunction and social factors. Brenn and sheikh observed that the factors associated with adverse outcome in stroke included male sex, unconsciousness, Glasgow coma scale of < 3, gaze palsy, pupillary changes and incontinence. The risk of death in first few days is best gauged by three clinical variables i.e. coma, paresis and incontinence, the indicators of severity of neurological dysfunction, along with cardiac variables like heart failure, atrial fibrillation and peripheral vascular disease. Patients with none of these factors are more likely to survive. Features suggestive of early brain stem dysfunction are indicators of poor outcome.5 Though the stroke related mortality is steadily declining in the west, it has been rising in India. This is due to the fact that the life expectancy has increased and urbanization has changed the life style. The total mortality observed in our study group was 34%. The patients with hemorrhage having a higher mortality of 56% and those with infarction having a lower mortality of 22.7%. The early mortality in stroke is reported to be around 20% in white population.1 Kazi et al6 reported an overall mortality, due to all causes, of 20% in all stroke patients. The cause stroke mortality observed in our study group was 34%, which is a little higher but comparable to other studies. The APACHE III score has been used effectively for prognosticating outcome in critically ill patients effectively.3 In the present study group, the sensitivity of this score at a cut off point of 40 was more than 90% (94% for hemorrhage and 90% for infarction). However, the specificity observed was a little lower. Among the various scoring systems in vogue for prognosticating outcome in stroke, Canadian neurological scale7 appears to be a powerful predictor of outcome i.e. the 4th month rate of death or disablement ranged from 10% in lowest risk group (< 70 years or CNS score of 7 or more) to 89% in highest risk group (> 70 years or CNS score of 4.5 or less). The National Institute of Health score also has a predictive accuracy of outcome around 80% in all patients8 We did observe that the likelihood of mortality increased as the score increased and the most noticeable increase was seen when the score was more than 40. Most of the scoring systems in vogue consider only the neurological deficit related parameters when evaluating these patients,7-9 while APACHE scoring system takes into consideration various other parameters like physiological variables, vitals, urine output, neurological score along with age related parameters and comorbid conditions which may have a significant impact on the outcome of these critically ill patients. Thus, this may be a better alternative and a good, effective predictor of short term outcome in cerebro-vascular accident patients. Conclusion Predicting outcome in stroke patients is difficult due to the variability in etiology presentation and underlying patho-physiology. APACHE III scoring system was found to be sensitive and reasonably specific in predicting short term, in - hospital outcome in critically ill patients having cerebrovascular accidents. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02081t1.jpg] [ni02081t2.jpg] |
| |||||||||

{kind=link}
{kind=link}