 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 282-285 CT Features of Intracranial Metastases of Unknown Primaries S.G. Srikanth, P.N. Jayakumar, H.S. Chandrashekar Departments of Neuroimaging and Interventional Radiology,
National Institute of Mental Health and Neurosciences,
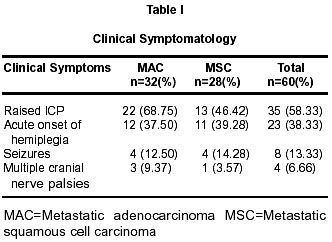
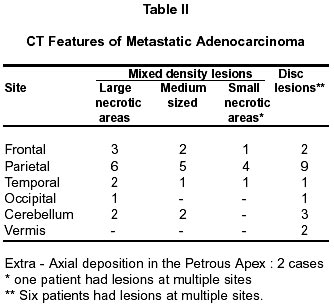
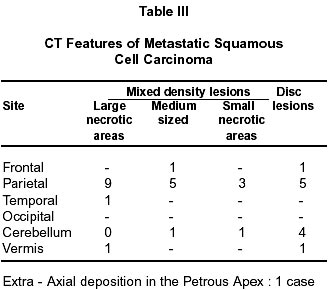
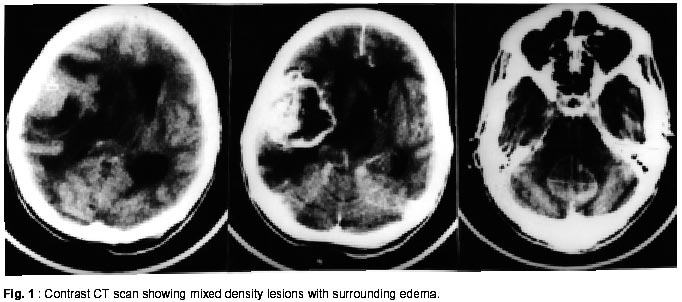
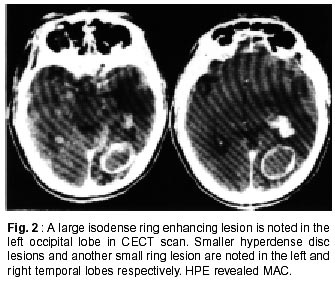
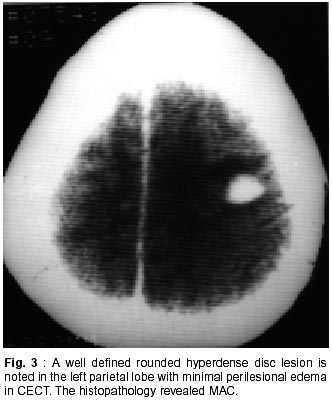
Bangalore - 560 029, India. Accepted for publication : 19th May, 2001. Code Number: ni02082 Summary Intracranial metastases of central nervous system are relatively common in patients with systemic cancer. Computed tomography (CT) scans of 60 patients of intracranial metastatic disease of unknown primaries, at the time of surgery, were retrospectively analyzed. These patients primarily presented with neurological dysfunction. They were operated upon for various reasons and histopathological diagnosis was obtained. There were 39 male and 21 female patients, with age range of 18 to 74 years. The common clinical symptoms were raised intracranial pressure without lateralization, acute onset hemiplegia and seizures. Multiple cranial nerve palsies were observed in 4 patients. Histopathologically the intracranial lesions consisted of metastatic adenocarcinoma (32 cases) or metastatic squamous cell carcinoma (28 cases). Among cases of adenocarcinoma, CT revealed solitary lesions in 17 and multiple lesions in 13 cases. Two had extraaxial deposition in the region of petrous apex. Out of squamous cell carcinomas, 17 lesions were solitary, while 10 were multiple and one had extraaxial deposition in the region of petrous apex. This study is unique as it consisted of CT features of intracranial metastases of unknown primary malignant disease elsewhere in the body. Key words : CT, Metastasis, Unknown primary, Brain. Introduction Metastatic disease to the central nervous system is a relatively common occurrence in patients with systemic cancer. The reported incidence of intracranial metastases with known systemic cancer varies.1 The site, type and incidence of intracranial metastases also vary according to the type of primary tumor. Lung carcinoma most often metastasizes to the brain parenchyma, while lymphoma or leukemia most frequently involve the meninges.2 Incidence of brain metastases may be higher when autopsy studies are considered. Jacobs et al reported that 6% of patients with lung carcinoma had brain metastases withoutsymptoms.3 We studied 60 cases of intracranial metastases, where primary was unknown. Material and Methods CT scans of 60 patients with confirmed intracranial metastases of unknown primary malignant disease at the time of surgery, were retrospectively studied. These patients primarily presented with neurological dysfunction. All the patients had contrast enhancing CT scans. There were 39 male and 21 female patients with age range of 18 to 74 years. All the patients had plain radiographs of the chest, ultrasound examination of the abdomen and biochemical investigation. Histopathological diagnosis was obtained in all after surgery. Results There were 60 patients with intracranial metastases, with unknown primary (IMUP) disease elsewhere in the body at the time of surgery. IMUP was common during 3rd to 5th decades of life. Preliminary chest radiographs and ultrasound examinations of the abdomen were normal including blood investigations. According to histopathalogic diagnosis, the intracranial lesions were metastatic adenocarcinoma (MAC) and metastatic squamous cell carcinoma (MSC). There were 32 cases of MAC and 28 cases of MSC. The clinical symptomatology of MAC and MSC is given in Table I. Raised ICP was the most common presenting symptom and was observed in 58% of patients. Acute onset hemiplegia mimicking a vascular episode was seen in 38%, seizures in 13% and involvement of multiple cranial nerves in 6% of patients. However, features of raised ICP were observed more frequently in patients with MAC (68%) as compared to MSC (46%). One patient of MSC gave history of recurrent episodes of right sided weakness of 10 months duration. CT scan showed a solitary lesion in the left parietal lobe (measuring 4.4x2.6 cm) with significant perilesional edema. Solitary lesions were more commonly encountered than multiple lesions in both MAC and MSC and together constituted 56.5%. Almost equal number of lesions were encountered in the supratentorial and infratentorial compartments in both MAC and MSC. Parietal lobe was the commonest site and was involved in 81% of patients, frontal lobe was involved in 22% of patients. There was no significant difference in the distribution of lesions in parietal, frontal and temporal lobes of brain between MAC and MSC. However, involvement of occipital lobe was observed in 2 patients of MAC only. The lesions on contrast enhanced CT scans in both MAC and MSC were broadly divided into: i) mixed density lesions with cystic components and ii) disc lesions. Mixed density lesions were again divided into 3 types: a) those with large cystic components measuring more than 5 cm, b) those with medium sized cystic components measuring 2 to 5 cm, and c) those with small cystic components measuring less than 2 cm. The CT scan features of both MAC and MSC are given in tables II and III. The disc lesions appeared iso to hyperdense on contrast enhanced CT scans and measured less than 2 cm in size, except in one patient where it measured 5 cm. Both mixed density and disc lesions were encountered in almost equal numbers in MAC and MSC. Mixed density lesions were the common type of lesions seen in both MAC and MSC (Figs. 1 and 2). These mixed density lesions were noted in 76% of our patients. Mixed density lesions with large and medium sized cystic components were noted in 71% of patients. Disc lesions were encountered in 20 patients, (33%) (Fig. 3). There was no statistically significant difference in the occurrence of these lesions among MAC and MSC. In two of our patients with disc lesions on CT scans, tuberculoma was diagnosed and patients were put on symptomatic treatment, however, there was no clinical improvement on follow up and repeat CT scan showed enlargement of these lesions with a morphological change to a mixed density lesions. Hydrocephalus was observed in 3 patients of MSC. Perilesional edema was significant in both MAC and MSC. Discussion Our study group consisted of 60 patients with unknown primary cancer elsewhere in the body at the time of surgery. The main presenting clinical symptoms of patients with brain metastases in the reported literature were: i) raised ICP, ii) neurological deficit and iii) seizures. The raised ICP in such patients rarely had any localizing value.1 Symptoms of brain metastases had a gradual onset; however, there may be acute presentation mimicking a vascular disease. In our patients, the most common complaints included raised ICP in 58%, acute onset of hemiplegia in 38% and seizures in 13%. Adults with brain metastases would present in early stages with raised ICP features compared to pediatric patients, because brain in children is more resilient as compared to adult brain.1 Brain metastatic lesions are destructive lesions which destroy the surrounding brain parenchyma resulting in varying degrees of neurological deficits and at the same time they are also irritative, causing seizures in such patients. Radiological and clinical diagnosis of brain metastases in a patient with a known systemic cancer is easy. However, diagnosis in a patient with no known primary cancer elsewhere in the body is difficult. Metastatic disease should be strongly suspected in patients with multiple cranial lesions.1 However, solitary lesions in patients with unknown primary cancer are less likely to be metastatic disease, but possibility of metastatic disease should be considered.1 Voorhies et al reported that solitary intracranial lesions may prove to be metastases in 15% of patients, with no known systemic cancer.4 Fifty six percent of patients in our study had solitary lesions as compared to 40% patients with multiple lesions. Until recently, CT scan was the primary imaging method of evaluation of patients with intracranial metastases. Of late there are many reports on the usefulness of contrast MRI in the evaluation of intracranial metastases. MRI with its multiplanar imaging capabilities, superior tissue contrast, elimination of bony artifacts and versatile parameters is an effective tool in the evaluation of such patients.5-8 None of our patients had MRI. 53-86% of patients with lung carcinoma may present with brain metastases as the initial sign of the disease.9 Histopathologically, the probale primaries in 50 patients of our group were as follows; lungs 20 (33%), gastrointestinal tract 15 (25%), ovary 7, two each with probable primary from breast, cervix and esophagus and one each with probable primary from kidney, thyroid and larynx. In the remaining 10 patients, no probable primaries could be detected. The surgical excision of solitary brain metastasis in patients with no known systemic cancer may increase the survival rate of such patients than in patients with known systemic cancer.1 It has been studied extensively that different primary tumors would take different time interval in spreading to brain. Primary from organs other than lungs would take longer time interval to metastasize to brain than lungs as hematogenic spread from other organs are shunted through lungs only. Lung carcinoma take 6-9 months to metastasize to brain.10-12 Conclusion The CT features of intracranial metastases include mixed density and disc lesions. There is no significant correlation between CT features and histopathological morphology. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02082t1.jpg] [ni02082t3.jpg] [ni02082f1.jpg] [ni02082f3.jpg] [ni02082t2.jpg] [ni02082f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}