 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 286-289 Thoracic Cord Compression Due to Ossified Hypertrophied Ligamentum Flavum P.N. Jayakumar, B. Indira Devi,* D.I. Bhat,* B.S. Das* Departments of Neuroradiology and Neurosurgery*,
National Institute of Mental Health and Neurosciences,
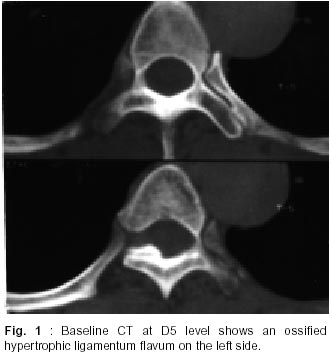
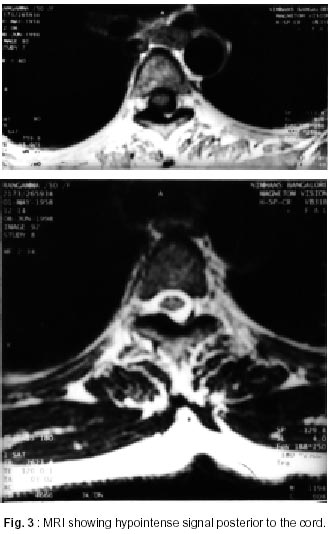
Bangalore - 560 029, India. Accepted for publication : 22nd November, 2000. Code Number: ni02083 Summary Ossified ligamentum flavum is increasingly appreciated as an important cause of thoracic myeloradiculopathy. Fifteen patients with age ranging from 30-61 years were studied. Fourteen presented with spastic paraparesis, and radiculopathy was the only complaint in one patient. Routine skiagrams and myelograms showed non-specific changes. Baseline CT and CT myelogram, however, documented the ossification of ligamentum flavum comprehensively. MRI was done in three patients. Multiple levels of the disease were seen in two cases. Four patients had ossified posterior longitudinal ligament. Thickened ligamentum flavum should be considered as an important cause of thoracic cord compression. Key words : Ossified ligamentum flavum, Thoracic cord compression, Paraplegia. Introduction Thoracic myeloradiculopathy is frequently due to tubercular or neoplastic disease. One of the less recognized causes is thickened ligamentum flavum. Since the first description by Yamaguchi and Isuruni, thickened ligamentum flavum is being gradually appreciated as an important cause of thoracic myeloradiculopathy.1-4 The pre-operative diagnosis of thickned or ossified ligamentum flavum (OLF) has become more definitive and easier with advances in imaging techniques. A series of fifteen patients of OLF, managed between 1987 to 1996, is reported. Material and Methods Fifteen patients (11 male and 4 female) with age ranging from 30 to 61 years were seen at the National Institute of Medical Health and Neurosciences between 1987 and 1996. All patients underwent routine skiagrams of the spine followed by watersoluble myelogram and twelve patients underwent contrast CT myelogram (CCTM). Baseline CT of the spine at the level of obstruction was done the following day. MRI was done in three patients. Table I summarises the clinical and radiological findings of the patients. Results Fourteen patients presented with paresthesias and stiffness in the lower limbs, while one patient had pain on the right side of the chest. The duration of symptoms ranged from 2 months to 18 months. Neurological examination revealed paraparesis and decreased posterior column sensations below the level of compression. OLF was suspected on routine skiagrams in two patients. Myelogram demonstrated an extradural compression in twelve patients. CCTM and nonenhanced CT showed ossification of the ligamentum flavum to be unilateral in three patients (Fig. 1) and bilateral in nine (Fig. 2). Multiple levels of block were seen both on myelogram and CT in two cases. Associated ossification of the posterior longitudinal ligament was seen in four patients. MRI demonstrated posterior compression due to calcified ligamentum flavum in three patients (Fig. 3). At surgery, the yellow ligament was found to be thickened and osseous. This was excised after laminectomy. First surgery did not improve the neurological status in two patients. The radiological studies were repeated and they showed an additional level of OLF proximal to the previous level examined by CT. Both the patients underwent repeat surgery. Laminectomy and excision of the OLF at the second level was done. No attempt was made to remove the OPLL in any of the three patients in whom it was detected. Histopathological examination showed an adenocarcinomatous secondary from an undetected primary in one patient. Discussion The ligamentum flavum (LF) is a yellow elastic ligament extending from the second cervical vertebra to the first piece of sacrum. It is composed of longitudinal network of elastic connective tissue and is routinely demonstrated on CT scans as an isodense structure, 2 to 4 mm thick, on the postero medial aspect of the laminae, contrasted by the adjacent fat. Thickening of this ligament may lead to various neuronal compression syndromes. This may be due to fibrosis of the ligaments, secondary to degenerative change or ageing.5 There may be in addition mucoid swelling and hyalinisation of the elastic fibrous connective tissue and buckling secondary to facet degeneration and spondylosis.4 Since the initial description of thoracic myelopathy due to ossified LF in 1964, there have been isolated reports in the literature.1,3,4 The thickened ligament may be calcified or ossified with appropriate attenuation on CT. The etiology of ossification of LF include trauma, diffuse idiopathic skeletal hyperostosis (DISH) ankylosing spondylosis,7,8 hemochromatosis, fluorosis and disorders of calcium and phosphorous. An interesting feature of our series was ossification of the thickened ligament in all our cases as compared to only two of the 7 cases of Stollman et al.4 None of our patients had associated causes of spinal stenosis such as disk protrusion or facet hypertrophy. This is significant as isolated ligamentum flavum thickening has been thought to have no clinical significance in the past.4 The causes of OLF in our series are diverse. One patient had fluorosis, another had diffuse ligamentous calcification suggestive of DISH and the third, adenocarcinomatous metastasis. The etiology in the other twelve patients is obscure. Though it is tempting to involve chronic repetitive trauma as a probable underlying cause, there was no overt evidence of degenerative or disk prolapse in any of them. The lower dorsal spine has greater mobility in flexion and extension. This may predispose to repeated trauma and calcification. Interestingly four patients had associated ossification of the posterior longitudinal ligament (OPLL) of the cervical spine. In an earlier report by Miyasaka et al, 14 patients with thoracic OLF and cord compression had associated cervical OPLL.2,5 All patients in this series presented with spastic paraparesis and sensory symptoms. Virani et al reported three patients presenting with backache.9 All of them were treated with laminectomy and excision of the ligamentum flavum following investigations. One patient in our series presented with pure radiculopathy due to thickening of the lateral part of LF. None of the patients of four series reported earlier presented with radiculopathy as the only clinical feature.2,4,5,9 Carcinoma of the prostate is known to metastasize through the vertebral plexus of veins. Secondary deposits are mostly in the axial skeleton. While extradural non ligamentous metastasis may occur, thoracic myelopathy due to ossified metastasis to the LF, as in one of our cases is extremely rare and interesting. One other patient had radiological evidence of sclerotic secondaries. He was referred for radiotherapy without surgery. The finding of multiple levels of thickening in two patients (at T4 and T11 levels in one and T6 and T8 levels in another) is significant. Recurrent symptoms or failure or post-operative improvement may be due to the presence of such additional levels of compression. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02083f3.jpg] [ni02083f1.jpg] [ni02083t1.jpg] [ni02083f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}