 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 295-300 Study of Factors Responsible for Recurrence of Seizures in Controlled Epileptics for more than 1½ Years After Withdrawal of Antiepileptic Drugs S.J. Lamdhade, G.M. Taori Department of Neurology,
Central India Institute of Medical Sciences,
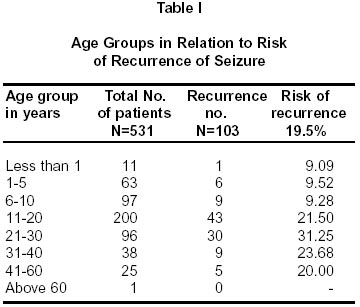
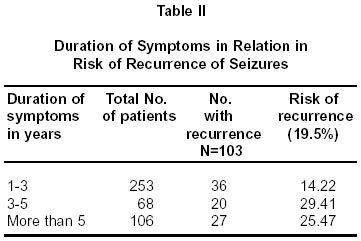
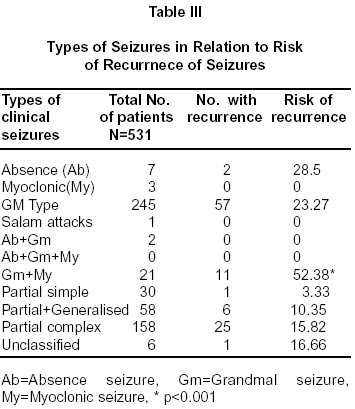
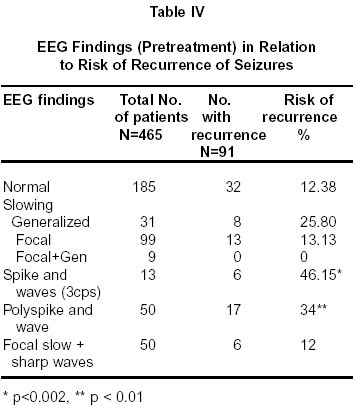
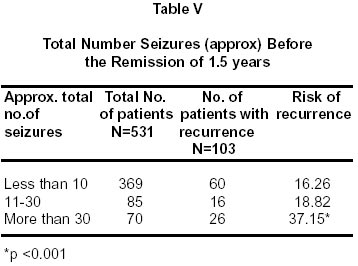
Nagpur-440 010, India. Accepted for publication : 12th October, 2001. Code Number: ni02085 Summary 531 epileptic patients, who had achieved remission mostly for 2 years or more were studied. The mean follow up period was 5 years. Recurrence was noted in 103 patients (19%) after gradual withdrawal of AED, over a period of 3-4 months. 424 patients (81%) did not have recurrence. The recurrence rate was influenced adversely by factors like adolescent age and later onset seizures, pre-treatment duration of symptoms more than 3 years, pretreatment precipitating factors like emotional stress, lack of sleep and meals (however, number in each group is small), positive family history of epilepsy, focal neurodeficit, absence and myoclonic plus grandmal type of clinical seizures, paroxysmal generalized spike and wave discharges and generalized short polyspike and wave discharges in the pretreatment EEG, atrophic changes on CT brain scan (in small numbers), head trauma at birth or later and hereditary factors as etiology of epilepsy, and more than 30 number of seizures before achieving the remission. Factors like, sex, frequency of seizures, period of remission i.e. two years or more and number of drugs used to achieve remission, did not have any significant adverse effect. However, in the last parameter 95% remission was achieved by one or a combination of two drugs (72% and 23% respectively). Key words : Seizure, Recurrence, Factor, AED withdrawl. Introduction Epilepsy is a world wide problem of diverse etiologies. In developed countries where advanced investigative facilities are available, 25-30% patients have seizure disorder of unknown cause, whereas in the developing countries this figure goes up to 60-75%.1 At our center, out of 1521 patients of epilepsy no cause was detected in nearly 64% of the patients. It is estimated that nearly 70% of all epileptics will go into long remission (more than 2 years) and about 43 to 50% will withdraw antiepileptic drugs (AEDs) successfully. It has been observed that once a substantial remission (24 months or more) has been achieved, the risk of further seizures is greatly reduced.1,2 Recently in a population based prospective follow up study of 9 years, Cockrell et al reported three year remission in 86% and five year remission in 68%.4 At a nine year follow up period, 3 year remission was noted in 68% and 5 year remission in 54%. In this study, patients with even single unprovoked as well as provoked seizure were included. In idiopathic etiology group, 5 year remission was noted in 69% and in remote symptomatic group it was 61%. Gowers in 1881 observed that an epileptic attack enhances the chances of recurrence of attack, thus, indirectly suggesting that every patient who has even a single seizure should be treated with AED.5 However, from the community based studies it has become clear that in some patients seizures stop even without any AED. Predictors of relapse have not yet been well defined. It is possible that in the newly diagnosed epileptics whose attacks are easily controlled and in those whom attacks are difficult to control behave differently.3 In the meta-analysis reported by Berg et al, the recurrence rate varied between 12% to 67%.6 On further analysis of various studies, these authors commented that in the untreated group of epileptics, recurrence was 25% at the end of first year and 29% at the end of second year. High rate of recurrence was seen with adolescent onset epilepsy, childhood epilepsy, and remote symptomatic seizures. Abnormal EEG was associated with increased risk of relapse in both children and adults. Chadwick suggested that age of onset, duration of epilepsy prior to the treatment, seizure type, etiology of epilepsy in a particular patient, abrupt versus slow withdrawal of drugs, and EEG - before initiating withdrawal of drugs could influence the recurrence.7 Number of seizures before therapy are one of the factors influencing the recurrence of seizures.8,9 In a quantitative hippocampal MRI study of 63 adult patients published by Paesschen et al, it was reported that in a newly diagnosed partial complex seizures, 10% showed hippocampal sclerosis.10 On further analysis, by hippocampal volume measurement and hippocampal T2 mapping, these authors concluded that the number of pretreatment seizures was an important indicator of recurrence. Patients with hippocampal sclerosis had difficult control of seizures. The present study was undertaken i) to study the recurrence rate of epilepsy after withdrawal of AED, after a remission period of 1½ to 3 years, in a hospital based population in India and ii) to evaluate the factors responsible for such recurrence. Material and Methods This study was conducted on epilepsy patients attending the neurology clinic of Central India Institute of Medical Sciences from 1984 to 1993 i.e. approximately 10 years. This is a long term retrospective analysis. Patients, who had achieved remission of 1½ years or more and in whom AED were withdrawn, were analyzed in this study. Amongst the group of patients with 'isolated' seizure, only cases who had either recurrence of seizure after the first seizure or who had 'flurry' of seizures or abnormal EEGs after the first seizure were included in this study. After withdrawal, these cases were followed carefully for atleast 2 years. For analysis, patients are divided in two groups i.e. 'No recurrence' (group A) and 'Recurrence' (group B). The data has been put to statistical analysis for comparison. Chi square test and p values are calculated using EPI info version 5 software. Patients of acute symptomatic seizures like head injury, CNS infections, metabolic disorders, tuberculoma, cysticercosis were excluded from this study. Results In the study period (1984 to 1993), 59,377 new patients were seen in the out-patient department. 10% of patients had epilepsy. Nearly 42% of the patients with epilepsy had follow up of atleast 6 months and of these nearly 60% had follow up of 2 or more years. It was observed that 40% of the patients with follow up of more than 2 years had total control of seizures, approximately 40% had 50-75% control of seizures and nearly 20% had no relief. During this period, 531 patients achieved remission of 2 or more years (except in 10 patients where remission was between 1½ to 2 years) in whom drugs were withdrawn. These 531 patients were divided into two groups. Group A : 'No recurrence group' (N=428, 81%) and Group B : 'Recurrence group' (N=103, 19%). There were 275 males in group A and 75 in group B. Gender had no relation with the recurrence. Patients were divided in eight groups according to their age (Table I). Significant association between recurrence was seen in age group of 20-30 years (Chi square=9.94, p<0.01). Duration of symptoms varied from less than one year to more than 5 years (Table II). Patients with long duration of epilepsy of three or more years had significant association with the recurrence (Chi square=9.60, p < 0.01). Frequency of seizure was divided into five groups i.e. i) 'frequent' - four attacks or more in a month, ii) 'infrequent'- attack not more than one in 3 months, iii) 'intermediate'- attacks in between groups 'frequent' and 'infrequent', iv) 'isolated'- single attack or flurry of attacks of two or more occuring within few hours and v) where frequency is not recorded. Patients with isolated single attack after recurrence of seizures during follow up, and patients having flurry of seizures in the first episode or abnormal EEG after the isolated seizure were put on AED. In the 'frequent' group (n=80), 18 had recurrence i.e. risk of recurrence was 22.5%; in the 'infrequent' group (n=193), 38 had recurrence i.e. risk of recurrence was 19.68%; in the 'intermediate' group (n=158), 33 had recurrence i.e. risk of recurrence was 20.88%; in 'isolated' group (n=93), 13 had recurrence i.e. risk of recurrence was 13.98%. In the group where frequency was not recorded (n=7) one had recurrence with recurrence risk of 14.28%. On statistical analysis no significant difference in risk of recurrence was noted in the various groups, eventhough in 'isolated' group tendency of recurrence was less. Emotional stress was precipitating cause of seizure in 7 cases. Four of them had recurrence, (risk of recurrence 57.14%). Recurrence in the 'lack of sleep' group and the 'meals group' was seen in 50% each. 31 patients had other precipitating factors including fever. They had recurrence in 16%. Risk of recurrence was 18% in cases with no risk factor (n=470). Number of patients in each of these groups was too small for the statistical analysis. Eighty six patients had positive family history for seizures sixty two were in group A (72.1%) and 24 in group B (27.9%). This association of positive family history was statistically significant for seizure recurrence (X2=3.98, p<0.05). Nine (1.13%) patients had focal neuro-deficit. Of these, 6 belonged to group A. Mild mental retardation was seen in twelve (2.2%); 10 of these belonged to group A. Only one patient had mental retardation and focal neurodeficit. Because of small number of patients with focal neurodeficit and mental retardation, statistical analysis was not possible. Mixed seizures (grandmal and myoclonic) had higher recurrence (p<0.001). It was also observed that risk of recurrence in patients in 'generalized epilepsy' group was higher than in patients in 'partial epilepy' group (p=<0.001) (Table III). Significant recurrence was observed in patients with spike and wave (p<0.02), and polyspike and wave discharges (p<0.01) (Table IV). One hundred forty-five patients (19%) had CT scan examination, of which 124 (85.5%) belonged to group A. Six (4.13%) patients had cortical atrophy (4 belonged to group A). Evidence of healed granuloma and other nonspecific changes were seen in 13 (9%) of these 12 belonged to group A and only one to group B. There was no significant correlation of seizure recurrence with CT scan findings. Recurrence after withdrawal of AED was seen in 70 cases, out of 401 patients without any cause i.e risk of recurrence was 17.46%. In various groups with known etiologies, the risk of recurrence varied between 14.29 to 50%. The recurrence was noted more frequently in patients with birth trauma. However, the number was small for statistical analysis. In other etiological groups no significant statistical difference was noted. Table V shows risk of recurreces with type of anticonvulsant used. After remission, AEDs were withdrawn at varying intervals. In 10 (2%) patients withdrawal was at 1.5- 2 years, in 128 (24%) at 2-3 years and in 393 (74%) after more than three years. It is seen that there is no relation of seizure recurrence to the duration of remission. It is observed that more the number of seizures before remission, greater is the chance of recurrence, and that 30 or more seizures prior to remission (Table V) had significant relation to relapse (p<0.001). Repeat EEG was done before drug withdrawal in 210 (39.54%) patients. It was observed that there was no correlation of prewithdrawal abnormal EEG findings and relapse. Amongst the patients in 'recurrence' group it is observed that relapse of seizures occurred at any time during the follow up, maximum (62%) in the first six months, 19% in the next six months and equal percentage after one year. Discussion Initiation and discontinuation of AED therapy in epilepsy has been the subject of study for more than five decades. Do the drugs simply elevate seizure threshold and reduce or abolish clinical seizures during a period of patient's life, which is determined by factors independent of drug therapy e.g. classification of patient's epilepsy or do they by suppressing the seizures, shorten the period during which the underlying epileptic disorder lasts? Gowers suggested 'the effect of a convulsion on the nerve center is such as to render the occurrence of another more easy, to intensify the predisposition that already exists.5 Thus, every fit may be said to be in part the result of those which had preceded it and the cause of those that follow it'. As per this observation and suggestion every patient even with one single unprovoked seizures, should be treated. However, now there are enough studies to indicate that a single unprovoked epileptic attack need not be treated. In fact, these days on experiencing one single unprovoked seizure, a person is not labelled as epileptic. Bora et al in their study of 147 adult patients of single unprovoked seizures, reported that patients who were not put on therapy, had overall recurrence rate of 41% by one year, after which the rate remained stable.11 Shinnar et al in their study 40% children with epilepsy reported cumulative risk of seizure recurrence of 29%, 37% and 42% at 1 year, 2 years, and 5 years intervals respectively.12 In the group of children with recurrence, 53% had recurrence in the first six months of the first seizure, 69% within first year and 88% within a period of 2 years. Only in 3% of cases, recurrence occurred after 5 years. In community based studies, it has been observed that a good number of patients even without therapy go in remission without any drug therapy. Further studies have shown that certain types of epilepsies have a far better prognosis than others.3 Gender did not contribute to recurrence of seizures in the preset study. Barring the neonatal seizure, childhood onset epileptics have better prognosis of long term remission. Epileptics with onset in adolescent and adulthood have higher chances of recurrence.8 Fenichel while commenting on this has suggested that children with epilepsy but otherwise normal are very likely to grow out of their epilepsy by 16 years age.13 These children are possibly having benign generalized epilepsies. In the present study as well, the recurrence after remission has been less common in childhood epilepsy as compared to adolescent and adult groups (Table I) Annegers et al noted a better rate of remission for patients with partial and generalized attacks if onset has been before the age of 20 years.14 In children the risk factors for recurrence of seizures after successful remission for more than 2 years, as enumerated by Gherpelli et al, included 10 or more than 10 seizures before control, an abnormal EEG in the year before withdrawal of AED, focal neurological signs or mental retardation or both and mixed seizure pattern.9 Camfield et al also noted higher chances of recurrence in patients with more than 20 attacks.8 Rodin emphasized that fewer and less frequent the seizures, better the prognosis for remission.16 In our study even though not restricted to children, the 'recurrence' was noted to be more in patients who had more seizures, the recurrence rate being low when attacks are less than ten in number (Table V). Chadwick in the review of literature on this subject has observed that the seizure type is important in recurrence of seizures.7 The recurrence rate reported in various types of clinical seizures have been grandmal type of seizure in 20-40%. Partial complex seizure is 40-60%, petitmal absence seizures is 20- 30%, complexes absence seizure is 35-67%, West or Lennox Gestaut syndrome is 50-65%. Combination of partial and grandmal seizures have poor prognosis. In the present study our figures tally very much with the above figures in the group of patients with grandmal and petitmal absence type of seizures (Table III). In patients with combination of grandmal and myoclonic type of seizures recurrence was in 52% (11/21 patients) cases in the present study. Others have also reported high figures in this group. The recurrence of seizures in patients with partial complex seizure in the present study has been low. Wirrel et al in their observations on long-term prognosis of typical childhood absences mentioned that as per literature most children go in life long remission. However, 33- 50% develop generalized tonic clonic seizures (grandmal) and 2.8 to 7.5% develop juvenile myoclonic epilepsy. In their own study of 82 children with follow up in 89% patients, 65% children were in remission, 17% were not taking drugs but continued to have seizures and 18% were taking drugs. Overall in their series with a mean follow-up period of 20.4 years, 15% of the children, who did not have remission, had developed JME. The factors that predicted 'lack of remission' included impaired cognitive functions at the time of diagnosis, absence status before or during AED therapy, development of generalized tonic clonic seizures or JME after starting AED, abnormal background activity in the initial EEG and positive family history of epilepsy in the first degree relatives. In the present study, there were 7 patients with absence attacks and only two had recurrence after withdrawal of AED (Table III). Duration of epilepsy before initiation of therapy has often been reported to be an important factor in the prognosis, Lesser the duration better the chances of remission. In the present study, same trend was noted; the lowest recurrence being in patients who presented within one year of start of epileptic attacks. Gowers stated that 83% of the patients would have seizure arrest if treated within one year. Annegers et al also showed that most patients who achieved remission did so early in the course of illness.14 Similar observation had been made by Shorvon and Reynolds.15 Etiologic factors could also play part in the prognosis of Epilepsy.7 Patients with unknown cause of epilepsy have been reported to have better prognosis. In our study as well, patients with unknown etiology had less recurrence after remission (17.46%). Patients with brain injuries, either at birth or afterwards in life, have more recurrence rate than cases with unknown cause. In the present study, patients with positive family history of seizures had higher recurrence rate. This could be because of the fact that certain types of epilepsies like absences, myoclonic, myoclonic and grandmal are more often hereditary in nature, where recurrence has been noted to be high. Adverse prognosis has been reported where epilepsy was associated with neurological and psychiatric deficit.7 In the present study, the number of patients with focal neurological deficit and/or mental retardation were few to drive any statistical difference between the two groups. Role of EEG in the prognostication of outcome in epileptics is not certain.7 Rodin felt that EEG alone cannot be used as criteria for prognostication but he did suggest that normalization of EEG during the course of illness was most important factor for remission.16 Anderson et al in their study of 244 children noted relapse in 37% of cases.17 Remission rate has been reported to be slightly higher in children whose last EEG recording before AED withdrawal was normal. These authors noted that children with irregular generalized spike and wave discharges before AED withdrawal had more chances of recurrence (67%) as compared to those with 'no epileptiform discharges (33%) and other types of EEG abnormality (33%). All children who were treated for one year and whose final EEG displayed generalized slow wave activity had recurrences. In the present study, the patients with i) generalized paroxysmal slow activity, ii) spike and wave type of generalized seizure activity, and iii) polyspike and wave type of generalized seizure activity had more chance of recurrence. The later two types of abnormalities are associated with clinical 'absence' and myoclonic and grandmal type of seizures, where the recurrence rate has been noted to be more (Table III). In the present study, pre-withdrawal normalization or nonnormalization of EEG did not show any difference in recurrence rate. In the present study, patients who had more seizures before the remission had higher rate of recurrence (Table V). However, it is interesting to note that the frequency of attacks did not have much bearing on the outcome except in cases of 'isolated' attacks where the recurrence rate was lowest. It should be emphasized that patients in 'isolated seizure group', were put on treatment if they had recurrence, had EEG abnormalities, had flurry of seizures in the 1st episode, had very strong family history or had abnormal CT scan. Any two of these factors were considered sufficient to put the patient on AED. 61% of patients had recurrence during withdrawal or after withdrawal within 6 months. 19% had recurrence within 1 year of withdrawal and in another 19% the recurrence was after 1 year of withdrawal of AED. Sex of patient, frequency of attacks, remission period and number of AEDs used for control of seizures did not have any significant effect on the recurrence rate. It is worth mentioning that in 95% of the patients seizure control could be achieved by one drug alone or with combination of two drugs. Acknowledgement We thank Dr. L.R. Kulkarni, Associate Professor of Statistics and Demography, IGMC, Nagpur for the statistical work. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02085t4.jpg] [ni02085t3.jpg] [ni02085t5.jpg] [ni02085t1.jpg] [ni02085t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}