 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
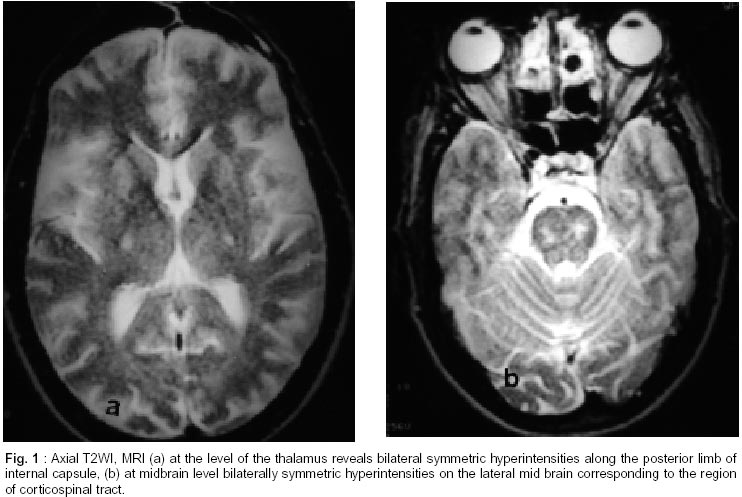
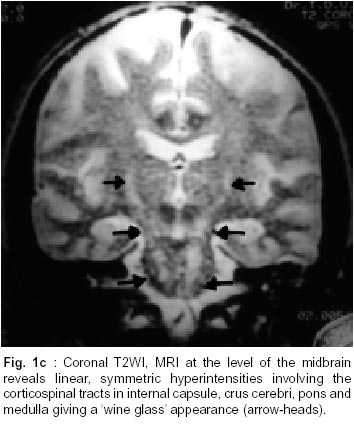
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 306-309 Case Report 'Wine Glass' Appearance : A Unique MRI Observation in a Case of Primary Lateral Sclerosis A. Kuruvilla, S. Joseph* Departments of Neurology and Neuroradiology*,
Sree Chitra Tirunal Institute for Medical Sciences and Technology,
Trivandrum - 695 011, India. Accepted for publication : 20th July, 2001. Code Number: ni02087 Summary Magnetic resonance images (MRI) in a patient with primary lateral sclerosis is described. T2WI, MRI of brain showed characteristic hyperintensities of the corticospinal tracts bilaterally, extending from the internal capsule to the brain stem - producing a 'wine glass' appearance on coronal sections, which has not been described so far to the best of our knowledge. Differential diagnosis of this interesting 'wine glass' appearance on MRI along with a review of the MR-signal abnormalities in motor neuron disease is discussed. Key words : Motor neuron disease, Primary lateral sclerosis, MRI, Wine glass sign. Introduction Motor neuron disease (MND) is a heterogenous group of disorders characterized by selective damage of the neural systems that mediate voluntary movement. The subgroups are defined clinically by the relative involvement of lower motor neuron or upper motor neuron functions, topography of the disease within the brain or spinal cord, and the age at onset. Amyotrophic lateral sclerosis (ALS) is the most common form of MND. Primary lateral sclerosis (PLS) is characterized by progressive upper motor neuron loss without any obvious clinical or pathological damage to lower motor neurons (LMN).1-3 PLS is rather uncommon, constituting only a few percent of all cases of MND including ALS. Whether it is an independent entity or a variant of ALS remains yet to be determined.4 Recently, MRI has documented white matter lesions in sporadic and familial MND.5-10 Although most of the previous reports have emphasized symmetric hyperintensity of the intracerebral corticospinal tracts in MND,5,6,11 in some, striking asymmetry in involvement of the corticospinal and spinocerebellar tracts have also been noted.12 We report a patient of primary lateral sclerosis, in whom, MRI of the brain revealed bilaterally symmetrical hyperintensity of corticospinal tracts extending from the internal capsule to the brain stem producing a characteristic 'wine glass' appearance. Case Report A 53 year old man presented with a slowly progressive weakness and stiffness of his right upper and lower limbs of 3 years duration. He had difficulty in speaking, associated with emotional lability. There was no cognitive decline, dysphagia, nasal regurgitation, sensory, visual or sphincter disturbance. He denied trauma or exposure to neurotoxins, radiation, or drug abuse. His family history was noncontributory. Neurological examination revealed normal mental status with emotional lability and brisk jaw jerk and facial reflexes. There was spastic dysarthria with a spastic tongue, without atrophy or fasciculations. Motor system examination showed bilateral, asymmetrical spasticity involving all limbs, more so on the right. The muscle power was MRC grade 3/5 and 4/5 in the right and left upper limbs respectively. The lower limbs had of normal power. All deep tendon reflexes were exaggerated with bilateral ankle clonus and Babinski sign. There was no sensory or cerebellar dysfunction. Routine hematological and biochemical investigations including chest X-ray were normal. Blood VDRL, HIV and antinuclear antibody were negative. The visual evoked potentials(VEPs) were normal. A paraneoplastic work-up including bone survey, computerized tomographic (CT) scan of the chest and the ultrasound of abdomen were also normal. A thorough clinical and electrophysiological examination including nerve conduction study (NCS) and electromyography (EMG) of all limbs did not reveal any evidence for a lower motor neuron (LMN) involvement. MRI of the brain revealed linear, bilaterally symmetrical hyperintensities (Fig. 1a-b, c) involving the corticospinal tracts in internal capsule, crus cerebri, pons and medulla on T2WI, giving a 'wine glass' appearance, seen in the coronal plane (Fig. 1c). The serial follow-up including EMG at 54 and 72 months into the illness had not shown any LMN involvement. On last follow-up, the patient was found to have a slight progression of spasticity involving all the limbs in addition to slight progression of spastic dysarthria. There was mild progression of weakness in the lower limbs. Discussion The history, physical signs and MRI in present case are consistent with a diagnosis of primary lateral sclerosis. The differential diagnosis of PLS is wide and it includes multiple lacunar infarcts of the brain, demyelinating disease like multiple sclerosis and persistent infection with human immunodeficiency virus (HIV myelopathy) and human T-lymphotrophic virus Type 1 (HTLV-1 myelopathy). Paraneoplastic syndrome and Sjogren's syndrome may at times resemble PLS.4 Our patient's clinical course and MRI were not suggestive of multi infarct state or MS.13,14 Although tropical spastic paraparesis has been associated with HTLV-1 infection, our patient's pseudobulbar features and profile of symptoms do not favour this diagnostic entity. The pathology of primary lateral sclerosis is limited to corticobulbar and corticospinal tracts (CST)1 as demonstrated in our case. A diagnosis of ALS cannot be excluded within 3 years of onset since LMN features may develop later.4 This case report underscores that a careful and detailed follow-up examination is crucial before PLS is diagnosed with certainty. ALS can present with a pure upper motor neuron (UMN) picture, however, it generally progresses more rapidly than PLS.4 The present case did not show any evidence for LMN dysfunction even at 72 month followup, thus excluding the possibility of ALS to a reasonable extent. Goodin et al5 reported symmetric areas of increased signal intensity extending from cortex through corona radiata, posterior limb of internal capsule, cerebral peduncle and pons on T2WI MRI in two patients with MND. Sales Luis et al6 also reported similar findings in 8 out of 20 patients with sporadic MND. None of the 11 healthy controls had an abnormal MRI.6 There has been anecdotal reports on MRI findings in sporadic MND from India. Bhat et al15 reported a 47 year old woman with amyotrophic lateral sclerosis (ALS) whose MRI revealed smooth, ovoid, bilaterally symmetric lesions in the frontal and parietal subcortical white matter, a finding which is different from our patient who showed linear, symmetric hyperintensities along the corticospinal tract extending from the internal capsule to medullary pyramids. Wallerian degeneration of the CST in motor neuron disease have been reported by various authors.7,8,16 In a study comprising MR images of brain of 50 ALS patients, Yagishita16 demonstrated abnormal foci in internal capsule in 9 patients, representing degeneration of the CST. Normal hyperintense signals in the internal capsule representing CST fibers were isointense to gray matter on T2WI and iso-or hypointense to white matter on proton-density weighted images. Midani et al,7 in a patient with juvenile ALS, showed bilateral hyperintensities along the corticospinal tracts extending from the corona radiata to the brain stem on T2WI MRI. These authors emphasized that these findings should be differentiated from the slight hyperintensities seen in the posterior limbs of internal capsules in normal population. In a study comprising 16 patients with ALS, 20 normal subjects and 113 controls with other neurological disorders, Segawa8 described high signal intensity on the posterior limbs of the internal capsules in all patients with ALS, 60% of the normal subjects and 73% of the disease controls. The T1WI showed high signal areas on the posterior limbs in 62% of the patients with ALS, but not in any of the normal subjects and the controls. Waragai17 reported high signal intensity in the intracranial CST on T1WI in 5 patients with ALS who showed pronounced UMN signs including spastic paraparesis, but not in controls. The author concluded that high signal intensity of the intracranial CST on T1WI may reflect severe pathology of the UMNs in ALS. In another study consisting of 80 patients with ALS and 80 age and sex-matched normal controls, Abe et al18 described hyperintense foci in the posterior limb of internal capsule in 52(65%) and 41(51%) cases respectively. On proton density-weighted images, while no control-subject showed increased signal intensities, hyperintense foci were observed in the posterior limb of internal capsule in 65% of ALS patients. Hofman et al,19 in a quantitative determination of the T2 relaxation time in 21 patients with ALS and 21 age and sex-matched controls, concluded that, the T2WI of patients and controls showed no statistical difference in any slice. There was no correlation between T2WI and type of presentation. However, proton-density images revealed a clearly high signal at CST in patients, and not in controls. It was specific but not sensitive for the diagnosis of ALS. Thus, a noninvasive technique like proton magnetic resonance spectroscopy combines the advantages of MRI with in vivo biochemical information. MRI findings in our patient were unique in that the corticospinal tract degeneration was seen symmetrically in a linear fashion giving a characteristic 'wine glass' appearance. We report this case to highlight this unique radiological appearance which may be a clue for suspecting this variant of motor neuron disease. A prospective neuroimaging evaluation with MRI of a larger cohort of patients with PLS would lead to better understanding of the radiological spectrum of this entity. These radiological findings might help to characterize the clinical and genetic heterogeneity in this group of disorders. Perhaps, other clinical entities mentioned earlier in the differential diagnosis may also give rise to similar MRI appearance, although not yet described. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02087f1a-b.jpg] [ni02087f1c.jpg] |
| |||||||||

{kind=link}
{kind=link}