 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 310-312 Case Report MRI in Subacute Combined Degeneration of Spinal Cord : A Case Report and Review of Literature S.G. Srikanth, P.N. Jayakumar, M.K. Vasudev, A.B. Taly,* H.S. Chandrashekar Departments of Neuroimaging & Interventional Radiology and
Neurology*,
National Institute of Mental Health and Neurosciences,
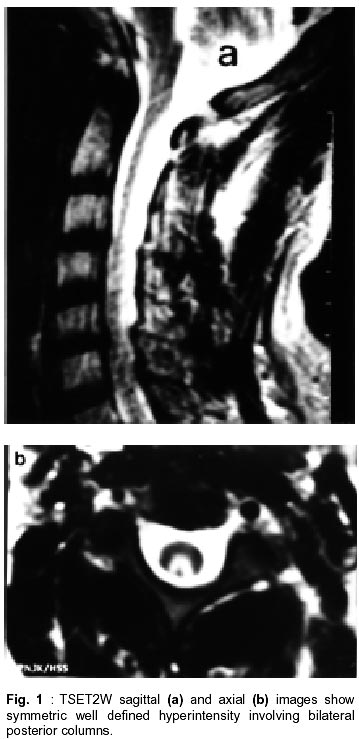
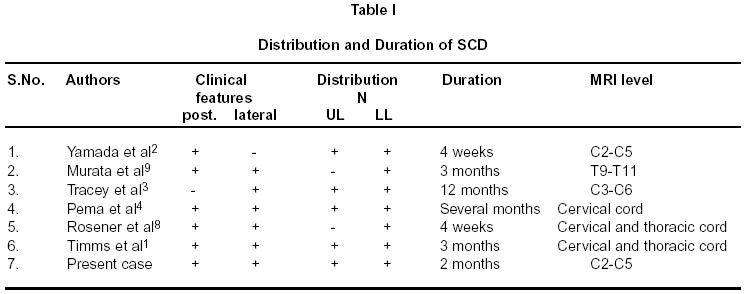
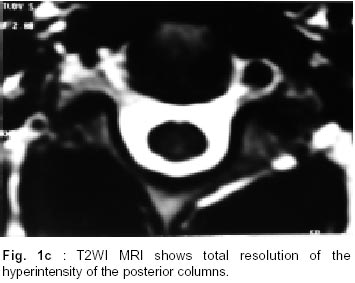
Bangalore - 560 029, India. Accepted for publication : 21st October, 2000. Code Number: ni02088 Summary A 56 year old man presented with acute onset posterior column and lateral spinothalamic tract dysfunction over a period of 15 days. MRI showed diffuse hyperintensity on T2WI involving the posterior columns.A diagnosis of subacute combined degeneration (SCD) of the spinal cord was considered and confirmed by laboratory findings. The patient showed complete recovery on B12 therapy. MRI lesion also compeletely resolved. Key words : Subacute combined degeneration, Spinal cord, Vitamin B12, MRI, Cord hyperintensity. Introduction Subacute combined degeneration (SCD) of the spinal cord is a complication of vitamin B12 deficiency, which is reversible if diagnosed and treated early. There is dysfunction of posterior and lateral spinothalamic tracts of the spinal cord. Both myelin sheaths and axons are destroyed mainly in the white matter of the spinal cord. MR signal changes characteristic of SCD have been reported, however, MRI improvement on therapy has not been recorded. We discuss clinial and MR features in SCD with review of the literature. Case Report A 56 year old man presented with acute onset of paresthesia involving both hands and feet of 15 days duration. He also complained of difficulty in walking and inability to feel the ground for the same period. Neurological examination revealed impairment of sensation of fine touch, pin prick, joint position and vibration in both hands and feet bilaterally. All the deep tendon reflexes were exaggerated, more so in the lower limbs. There was no evidence of motor weakness. The initial laboratory investigations revealed dimorphic anemia which was confirmed on bone marrow biopsy. Visual evoked potential and brain stem evoked potential studies were within normal limits. Gastric endoscopy and biopsy revealed changes of atrophic gastritis. Workups for infections, para infectious myelitis, multiple sclerosis and connective tissue disorders revealed no abnormality. Folic acid and vitamin B12 levels in the serum were 7 micrograms and 75 picograms respectively. A cervical MR examination was performed. T2WI demonstrated diffuse hyperintensity in the posterior part of the spinal cord extending from C2 to C5 with cord edema. The visualised upper dorsal cord was normal. The axial images revealed involvement of posterior columns bilaterally. There was no enhancement of the lesion on contrast studies. The image findings were consistent with earlier reports of SCD.1-5 The patient was treated with parenteral administration of vitamin B12 and oral folic acid. At 10 months follow-up, he had improved significantly and MRI revealed total resolution of cord abnormality. Discussion Pernicious anemia, an antibody mediated intrinsic factor disorder, is the most common cause for vitamin B12 deficiency in western countries. However, in India, alcoholism, malnutrition and ileocecal tuberculosis are the common causes. The most common manifestations are hematologic, gastrointestinal and neurologic. The pathogenesis of neurological complication of vitamin B12 deficiency is not clear. However, deficiency state results in decreased activity of cobalamin-dependent methylcobalamin esterase enzyme with the resultant elevated levels of methylmalonic acid, which is toxic to myelin.6 Both myelin sheaths and axons are destroyed mainly in the white matter of the spinal cord. Similar clinical features and MRI findings have been described in nitrous oxide toxicity.7 All these patients had undergone surgical procedures for various reasons with nitrous oxide as the anesthetic agent. These patients were found to have vitamin B12 deficiency state unknown at the time of surgeries. The nitrous oxide is known to interfere in the activity of methylcobalamin, the active form of Vitamin B12 resulting in the accumulation of methylmalonic acid which is toxic to myelin.1,4,6,8 Our patient had routine T1WI and T2WI in axial and sagittal planes. The T2WI demonstrated diffuse hyperintensity in the cervical cord involving the posterior column extending from C2 to C5 levels (Fig. 1a and b). This case also failed to demonstrate lateral column involvement on MRI although clinical involvement of the same was noted. Others also reported similar findings on MRI.1,4,9 We reviewed the literature of clinical features and MRI findings in patients with SCD, as given in Table I. Six patients, including ours, had involvement of cervical spinal cord, one had thoracic and another had contiguous involvement of cervical and thoracic cord. MRI failed to demonstrate lateral column abnormality in all the patients including ours. However, some authors have demonstrated involvement of lateral column and atrophy of the cord in patients with SCD.10,11 Clinically, six patients had dysfunction of both upper and lower limbs. Two patients had only lower limb involvement and none had only upper limbs symptoms. All but one patient had both posterior and lateral columns dysfunction and one had only posterior column dysfunction. Four patients including ours presented during acute phase of the iliness, two during 9-12 months and one presented one year after the onset of the illness. All the patients received parenteral vitamin B12. However, our patient received oral folic acid in addition. The follow-up of such patients ranged from 2-10 months. Two patients including the present case showed dramatic response to treatment and at 10 months follow-up their MRIs had become normal (Fig. 1c). Conclusion SCD is a known complication of vitamin B12 deficiency, which usually is reversible, if diagnosed and treated early. MRI demonstrate involvement of the cervical cord in majority of the patients, although the pathology begins in the thoracic cord. MRI also demonstrates contiguous involvement of multiple segments of the cord. The cord abnormality can resolve without evidence of cord atrophy on MRI, if treated early. We presume that demonstration of involvement of lateral columns in all the patients is beyond the resolution of current MRI scanners. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02088t1.jpg] [ni02088f1c.jpg] [ni02088f1a-b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}