 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 313-315 Delayed Extradural Hematoma : A Case Report J.P. Alappat, Baiju, Praveen, K. Jayakumar, P. Sanalkumar Department of Neurosurgery,
Medical College and Hospital,
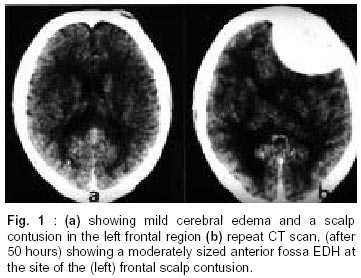
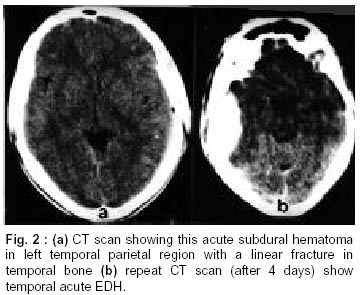
Calicut, Kerala, India. Accepted for publication : 24th January, 2001. Code Number: ni02089 Summary Three patients of delayed extradural hematoma (EDH) were seen in the last one year among forty eight consecutively treated cases of EDH. All the three hematomas were evacuated. Awareness of this entity and a high degree of vigilance are strongly recommended to detect such cases. Repeat CT should always be done, especially after decompression by either surgical or medical means, recovery from shock or whenever there is evidence of even minimal bleeding under a skull fracture on initial CT scan. Key words : Extradural hematoma, Delayed onset. Introduction Delayed extradural hematoma (EDH) can be defined as one in which the initial CT scan done within first 24 hours after trauma is normal or shows an insignificant EDH and subsequent CT scan shows a significant EDH. Delayed EDH is rare and, just like 'delayed intracerebral hematoma', is detected by the increasing use of repeat CT scanning. Case Reports Case 1 : A 16 year old boy was hit by a scooter. He was unconscious for a period of half an hour and vomited thrice. On examination in the casualty, the patient was conscious, and moved all 4 limbs. His pulse was 82/min and BP 130/80 mm of Hg. CT scan done within 6 hours showed mild cerebral edema and a scalp contusion in the left frontal region (Fig. 1a). There were no fractures. He was observed in the ward and was given intra-venous mannitol (100 ml twice a day). Patient was alright for 48 hours after accident. On the 3rd day, he started vomiting again, his GCS dropped to 12/15 and he developed bradycardia. Repeat CT scan, after 50 hours of first CT, showed a moderately sized anterior fossa EDH at the site of the (left) frontal scalp contusion (Fig. 1b). By the time he was taken for surgery, GCS had dropped to 9/15. There was no history of bleeding disorder. His coagulation work up was normal. Evacuation of the hematoma was done through left frontal craniotomy. There was no underlying fracture or bleeding vessel. He recovered fully and was discharged on the 7th postoperative day. Case 2 : A 27 year old man was involved in a road traffic accident. There was no history of loss of consciousness or vomiting. On examination in casualty, patient was fully conscious, with a GCS of 15/15, pulse 100/min, and BP 90/60 mm/Hg. He had fracture of the right femur. After correction of the shock by fluids and stabilization of vital signs, he was taken for a CT scan. CT showed a thin acute extradural hematoma in left temporoparietal region with a small air bubble (accident-CT interval : 8 hrs). Since he was fully conscious, he was managed conservatively with antibiotics. No decongestant therapy was given since there was only a thin acute EDH. On the 3rd day, he deteriorated in consciousness level (GCS 13/15). His coagulation profile was normal. A repeat CT scan (1st CT - 2nd CT interval : 62 hrs) showed a moderate sized temporoparietal EDH, at the site of thin EDH. Evacuation of the hematoma was done. There was no underlying fracture or bleeding vessel. He was discharged on 7th postoperative day. Case 3 : A 20 year old boy was admitted with a history of fall from a staircase. There was history of loss of consciousness for nearly half an hour. He had repeated vomiting and was disoriented. His pulse was 80/min; BP-130/70 of mm/Hg and GCS 13/15. Pupils were equal and reacting. Initial CT scan showed thin acute subdural hematoma in the temporoparietal region with a linear fracture in temporal bone and a small frontal contusion (accident CT interval-8 hours). He was put on mannitol and anticonvulsants but did not show the expected improvement even after 3 days. So a repeat scan was done on the 4th day which showed a moderate sized temporal acute EDH (Fig. 2) (1st CT-2nd CT interval - 72 hours). His coagulation profile was normal. Evacuation of the hematoma was done. There was an underlying fracture. He slowly recovered and was discharged on the 10th post-operative day. Discussion EDH may be classified into two clinical groups i.e. acute and subacute. Acute cases include patients with neurological deficits who need surgery within 3 days of trauma. Vast majority of these patients undergo surgery within 24 hours. Subacute cases are less well defined and include patients who present 4 days or longer after injury.1-4 Delayed traumatic EDH is considered to be uncommon and in some large series is not mentioned at all.5,6 Nevertheless, the incidence of delayed EDH has been reported to be 8-10%.8 Delayed EDH can be diagnosed only by scanning the patient twice. Otherwise it would be impossible to distinguish between delayed bleeding and late presentation of symptoms as in subacute and chronic SDH. The ever increasing indications for CT scanning in head injured patients have disproved, at least partly, the statement that EDH formation achieves near maximum size minutes after trauma. The fundamental causes of delayed traumatic EDH are not only the source of bleeding or the extension of the separation of the dura mater from inner surface of calvaria, as was shown in acute experimental models by Ford and MeLaurin,9 but also include the disturbance of the equilibrium in the brain and the hemostatic effect of the intracranial pressure. Low ICP, high BP or rapid correction of hypotension acting concurrently or in isolation favour the production of a delayed EDH, especially at areas already injured, such as under a skull fracture.2,7,8 It is well known that low ICP can bring about intracranial bleeding by itself without trauma as in cases of extracerebral hemorrhage complicating shunt surgery, ventricular and subarachnoid drainage, spinal anesthesia, posterior fossa and spinal intradural operations. ICP monitoring is a useful tool to detect such delayed EDH. In the 1st case possible cause could have been the mannitol therapy and in the 2nd case, the fracture femur and hypotension. In 3rd case, the possible explanation could be the fracture of the temporal bone and bleeding from the fracture site. Neurological deterioration is a reliable indicator to ask for a repeat CT scan, but if the contributory factors which favor a delayed traumatic extradural hematoma are present, a delayed EDH can be suspected as the reason for determination. The contributory factors for formation of EDH include (i) hyperventilation, (ii) mannitol, (iii) pentothal (iv) CSF leak-otorrhoea or rhinorrhoea, (v) surgical decompression, (vi) low blood pressure or shock. This is especially true in cases with a skull fracture contralateral to the original hemorrhage or signs of bleeding underneath any previously detected skull fracture. In conclusion, awareness of an entity of delayed EDH will help us to think about that possibility when a head injured patient deteriorates, and a timely intervention gives an excellent result just like in case of an acute extradural hematoma. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02089f2.jpg] [ni02089f1.jpg] |
| |||||||||

{kind=link}
{kind=link}