 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 316-318 Case Report Epidural Abscess and Staphylococcus Aureus Endocarditis - A Rare Association P. Malhotra, S. Jain, S. Kumari, Paramjeet,* S. Varma Departments of Internal Medicine and Radiodiagnosis*,
Postgraduate Institute of Medical Education and Research,
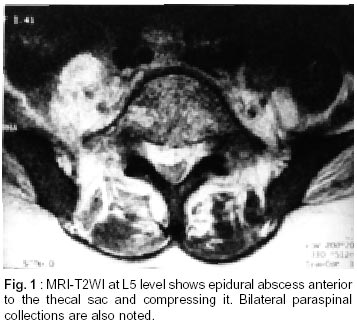
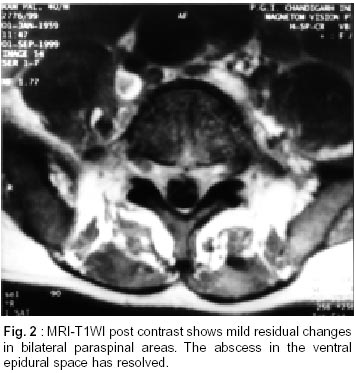
Chandigarh - 160 012, India. Accepted for publication : 30th January, 2001. Code Number: ni02090 Summary Epidural abscess is a relatively uncommon disorder. Although the surgical management is the mainstay of treatment, there are case reports of it being managed conservatively in selected patients. We report a patient who presented with quadreparesis due to epidural abscess and had infective endocarditis due to Staphylococcus aureus septicemia. Both epidural abscess and infective endocarditis were managed conservatively with intravenous antibiotics given for four weeks, with complete recovery of patient. Key words : Epidural abscess, Infective endocarditis, Staphylococcus aureus, Spinal, Treatment. Introduction Epidural abscess is a surgical emergency that requires immediate decompression.1 The common causes of epidural abscess are interventions in the spinal space, and spread from nearby bone or soft tissues.2 Conservative management of epidural abscess is reserved for patients with a poor surgical risk or in those without any neurological deficit.2 Association of epidural abscess with infective endocarditis has rarely been described.3-7 We present here a case of epidural abscess associated with Staphylococcus aureus endocarditis. Case Report R, 30 year old male, was admitted with complaints of radicular pain radiating to the legs after lifting a heavy load 7 days ago, and quadriparesis of 3 days duration. The weakness started from lower limbs and progressed to involve the upper limbs. He also had constipation and urinary retention. He developed high-grade fever on the day of hospitalization. On examination, he was febrile (39.5°C), with pulse of 130/min and blood pressure of 120/60 mm Hg. His cardiovascular and abdominal examinations were unremarkable. Examination of chest revealed coarse crepitations and bronchial breath sounds in left infrascapular area. Neurological examination revealed hypotonia and a power of 3/5 in upper and lower limbs. Deep tendon reflexes were absent and the plantars were extensor. No sensory loss could be demonstrated. Investigations showed a hemoglobin of 12.9g/dl and a total leukocyte count of 3.73 x 109/l with predominantly polymorphonuclear response. Renal and liver function tests were normal. Chest Xray showed features of left lower zone consolidation. Two consecutive blood cultures grew methicillin sensitive Staphylococcus aureus. Magnetic resonance imaging (MRI) of spinal region showed epidural and paraspinal abscess from cervicodorsal to 5th lumbar vertebra (Fig. 1). Transthoracic echocardiography showed 3x4 mm vegetation on anterior mitral leaflet. There was no underlying valvular lesion. Ultrasound guided drainage was attempted from paraspinal abscess and few drops of pus were drained. Pus showed gram-positive cocci; the culture, however was sterile. His HIV serology was nonreactive. The patient was administered injectable cloxacillin and amikacin. He was planned for decompressive surgery, however he showed improvement in his power within 48 hours and surgery was withheld. Subsequently, daily monitoring of the patient's muscle power and other parameters was done. The antibiotics were continued for 4 weeks and patient showed gradual improvement in his fever and power. A repeat MRI of cervicodorso- lumbar region after four weeks of antibiotics showed resolution of abscess (Fig. 2). A repeat echocardiography at four weeks did not show any vegetations and patient was well at 6 months of follow-up. Discussion Epidural abscess is a rare clinical condition with an estimated incidence of 0.2-2/10000 hospital admissions in the western world.8 The usual causes consist of intervention in the spinal space (lumbar puncture, any surgery), hematogenous spread from skin, soft tissues, direct extension of vertebral osteomyelitis, abdominal abscesses, infection of mediastinum and rarely infective endocarditis.1,2 The cause of epidural abscess in the present case may be a minor spinal trauma while patient was lifting a heavy load on his back which might have led to development of epidural hematoma.9 Blunt trauma is reported to precede the symptoms of spinal epidural abscess in 15-35% of cases.10 It is postulated that trauma may result in the formation of an epidural hematoma which subsequently becomes infected. The exact source of infection remains occult in 12-50% of cases.1 Staphylococcus aureus is widely prevalent in healthy individuals. An effective host response is necessary to prevent infection by this organism. A break in the natural barrier of body e.g. trauma, thus can lead to infection.11,12 However, of all the infections caused by Staphylococcus aureus in the body, epidural abscess is reported very rarely. In a hospital based study of 162 cases of Staphylococcus aureus infection, Musher et al reported only three cases of epidural abscess.11 The exact reasons for such a low involvement of epidural space by Staphylococcus septicemia is not known. It is likely that the present case developed Staphylococcus epidural abscess after the spinal trauma which lead to Staphylococcus septicemia and secondary involvement of lungs (pneumonia) and the heart (endocarditis). This patient did not have any heart murmur or other clinical features to suggest underlying heart disease at admission and during hospitalization. The vegetations were seen on normal valve and repeat echocardiography after 4 weeks also did not reveal any underlying heart disease. Thus, this patient had normal valve infective endocarditis. The study by Bayer et al in Staphylococcus septicemia patients found that 18% of patients without clinical evidence of infective endocarditis can have echocardiographic evidence of endocarditis.12 The treatment of epidural abscess usually consists of decompressive laminectomy and debridement along with antibiotics.8 However, there are case reports of it being managed conservatively.13 The conservative management is reserved for poor risk patients with concomitant medical problems, patients with extensive epidural abscess (from cervical to lumbar region), patients with severe loss of neuronal functions and patients with complete paralysis lasting for more than three days, and patients with no neurological deficit.1 The present case shows that conservative management can be tried in few patients of epidural abscess who show improvement in initial 48 hours, with close monitoring of neurodeficit. However if anytime neurodeficit worsens, decompression surgery should be done immediately. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02090f2.jpg] [ni02090f1.jpg] |
| |||||||||

{kind=link}
{kind=link}