 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 319-321 Case Report Wasp Sting Induced Neurological Manifestations A. Sachdev, M. Mahapatra, S. D'Cruz, A. Kumar, R. Singh, S.S. Lehl Department of Medicine,
Government Medical College and Hospital,
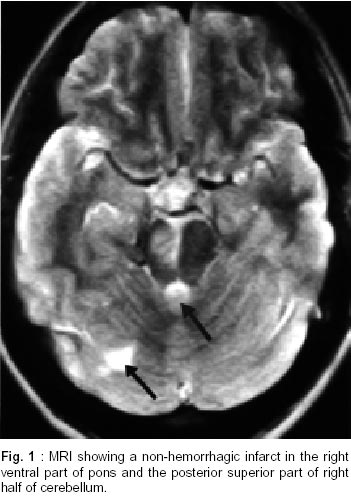
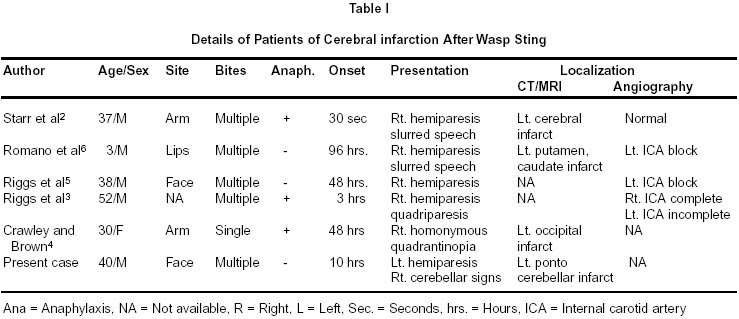
Chandigarh - 160 047, India. Accepted for publication : 5th January, 2001 Code Number: ni02091 Summary Wasp stings generally cause local reactions like pain, wheal, flare, edema and swelling, which are generally self-limiting. Multiple stings can lead to vomiting, diarrhea, generalized edema, dyspnea, hypotension, collapse, renal failure or death. Unusually, they may cause serum sickness, vasculitis, neuritis or encephalitis.We report a case of a 40 year old male who developed focal neurological deficit 10 hours following a wasp sting, which was confirmed to be ponto-cerebellar infarction on MRI scan, and recovered within five days. Key words : Hymenoptera sting, Vasculitis, Stroke. Introduction Wasp stings are commonly encountered worldwide.1 Various manifestations after wasp sting have been described. Local reactions are common. Unusually, manifestations like vomiting, diarrhea, dyspnea, generalized edema, acute renal failure, hypotension and collapse may occur. Rarely vasculitis, serum sickness, neuritis and encephalitis have been described which generally develop days to weeks after a sting.2-7We report a case of a 40-year-old male who developed left sided hemiplegia along with right side facial nerve palsy accompanied by right-sided cerebellar signs following a wasp sting. Case Report A 40 year old male laborer presented with history of sudden onset weakness of left half of body, slurring of speech and deviation of angle of mouth to the left side of five days duration. The weakness developed 10 hours after a wasp sting on the right side of face, which was followed by a local reaction in the form of swelling, pain and redness. There was no history of seizures, altered sensorium, urinary and bowel disturbances or sensory symptoms. He was a nonsmoker and not a known diabetic or hypertensive. There was no history of previous wasp or insect bite. Examination revealed a conscious person with spastic dysarthria. There was right nuclear 7th cranial nerve palsy along with left hemiparesis, power of grade II on left side, left hyper-reflexia and extensor plantar response. Cerebellar signs were present on right side. He had transient mild hypertension. There was no carotid bruit or cardiac murmur. Rest of the systemic examination was normal. Investigations revealed hemoglobin of 11.8 g/dl and TLC of 11,800/mm3. DLC revealed polymorphs-79% and lymphocytes-21%. Platelets were 2.8x105/mm3. Prothrombin time and activated partial thromboplastin time were 13 seconds and 39 seconds respectively. Fasting blood sugar was 87 mg/dl. Lipid profile was normal (serum cholesterol 180mg/dl, LDL 151mg/dl, VLDL 32mg/dl, HDL 55mg/dl, triglycerides 190mg/dl). Renal and liver function tests were normal. Antinuclear antibody and VDRL were negative. ECG and chest X-ray were normal. Echocardiography and carotid doppler revealed no abnormality. CT scan done 24 hours after the sting revealed a non-hemorrhagic infarct in the right ventral pons and the posterior superior part of right half of cerebellum which was confirmed by MRI (Fig. 1). He was managed conservatively with anti cerebral edema measures along with aspirin. Over the next five days, power in the limbs improved to normal; however there was persistence of cerebellar signs and dysarthria. On follow up two months later, he had showed further improvement. Discussion Hymenoptera stings occur quite frequently. These insects have a characteristic habit of defending their colonies and include apids (bees and bumble bees), vespids (wasps, hornets and yellow jackets) and ants. Their venoms contain a wide array of amines, peptides and enzymes that are responsible for local and systemic reactions. While bees lose their venom apparatus in the act of stinging and subsequently die, vespids can sting numerous times in succession. The venom of different species of hymenopterans is biochemically and immunologically distinct.1 Mixtures of low molecular weight compounds such as serotonine, histamine and acetylcholine and several kinins mediate direct toxic effects. Enzymes like hyaluronidase and phospholipases allow the venom to spread. There is only little cross-sensitization between bees and wasp venom. Generally, these stings cause local reactions like immediate pain, wheal and flare reaction, which settle within a few hours. Stings from accidentally swallowed insects may induce life-threatening edema of the upper airways. Multiple stings can lead to vomiting, diarrhoea, generalised edema, dyspnoea, rhabdomyolysis, intravascular hemolysis and renal failure. Neurologic reactions to wasp stings are very uncommon, delayed in onset and fatal in outcome. A variety of peripheral and central nervous system lesions have been described.2 The cerebral lesions may consist of edema, hemorrhage, infarction, necrosis and degeneration. There have been only five case reports of cerebral infarction due to wasp sting2-6 (Table I), and another case of hereditary hypoplasminogenemia, who developed recurrent arterial thrombo-embolism following wasp sting; however, its details are not available.7 In an unusual presentation, a 52 years old male presented with a severe anaphylactic reaction after a wasp sting. Few hours later, he developed left hemiparesis with slurred speech. Three and a half weeks later, he became obtunded and developed quadriparesis. Angiography studies confirmed occlusions of both right and left internal carotid arteries.3 Our patient did not have any delayed deficit and showed improvement on follow up. The onset of neurological symptoms varies from 30 seconds to 96 hours as reported in literature. Barring one case, neurological manifestations followed after multiple stings. The postulated mechanisms include vasoconstriction, platelet aggregation, and retrograde stimulation of superior cervical ganglion leading to occlusion of terminal internal carotid artery.4,5 The point of interest in this case report is the occurrence of a ponto-cerebellar infarction in a normal healthy person following a wasp sting, which is a very unusual complication and to our knowledge, this is the seventh case of this type. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02091f1.jpg] [ni02091t1.jpg] |
| |||||||||

{kind=link}
{kind=link}