 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 322-325 Case Report Crossed Cerebral - Cerebellar Diaschisis : MRI Evaluation A. Chakravarty Department of Neurology,
Vivekananda Institute of Medical Sciences,
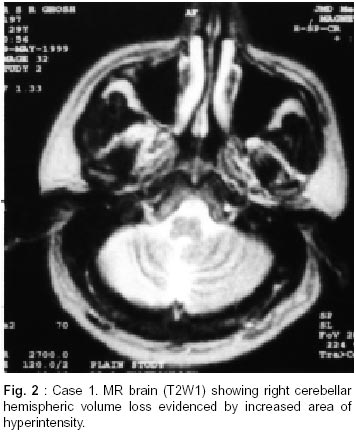
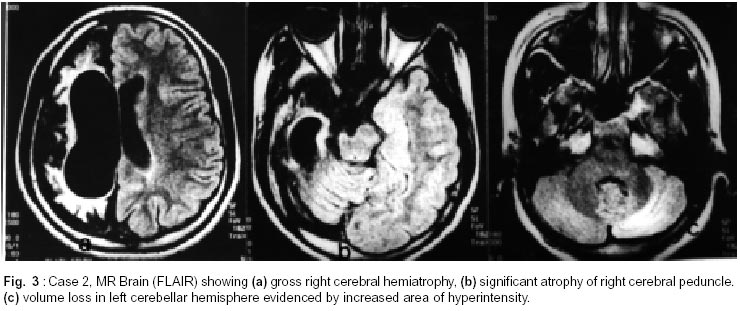
Calcutta, India. Accepted for publication : 7th February, 2001 Code Number: ni02092 Summary MRI, done later in life, in two patients with infantile hemiplegia syndrome showed significant volume loss in the cerebellar hemisphere contralateral to the side of the affected cerebrum. The cerebellar volume loss seemed to correlate with the degree of volume loss in the contralateral cerebral hemisphere. These observations provide morphological evidence of the phenomenon of crossed cerebral-cerebellar diaschisis (CCD). Functional neuroimaging studies in support of the concept of CCD has been critically reviewed. Key words : Crossed cerebral, Cerebellar diaschisis. Introduction Diaschisis in neurology signifies reduction of function of a part of the brain following the interruption at a remote site of an afferent pathway which normally supply background excitation to the neurons in that part, keeping them in a state of low activity.1 The concept was first introduced by von Monakow who described diaschisis corticospinalis (progression of functional depression of the spinal cord following an injury to the motor cortex); diaschisis commisuralis (functional depression of the contralateral cerebral cortex after injury to cortex of one hemisphere); and diaschisis associativa (depression of function in intact cortical areas adjacent to the site of a cortical injury).1 Each cerebellar hemisphere is intimately connected to the contralateral cerebral cortex through feed-back circuits, needed for smooth execution of motor function. The concept of crossed cerebral cerebellar diaschisis following injury (usually vascular) to the motor cortex of one cerebral hemisphere was popularised by Baron and his colleagues.2 In the present communication, the author has highlighted MR evidence of structural changes induced in the cerebellum, as a result of such changes in vascularity and metabolism, secondary to injury to the contralateral cerebral hemisphere in two patients with infantile hemiplegia. Case Report Case 1 : SRG, 30 years male, was first seen in May 1999 for control of refractory complex partial seizures. The seizures were characterized by speech arrest, right upper limb jerking and brief periods of loss of consciousness. In early childhood (< 1 year of age), he had an episode of recurrent seizures (probably right focal motor with secondary generalization) following which he developed a right hemiparesis, which persisted till date. Only infrequent seizures occurred till the age of 10 years but thereafter the seizure frequency increased considerably inspite of anticonvulsant therapy. He had remained mentally subnormal (verbal IQ <60) and never attended school. He had a spastic right hemiparesis with the right hand considerably smaller in size than the left. But he remained mobile independently. His seizures were controlled following treatment with carbamazepine, clobazam and topiramate. MRI revealed (Fig. 1 and 2) left cerebral hemisphere volume loss with widening of the sulci, specially in the sylvion area and compensatory dilatation of the lateral ventricle on the same side. The left side of the brain stem was flattened. The right cerebellar hemisphere showed moderate volume loss with widening of the sulci and thinning of the folia. Total hemispheric volumetry was not possible with the scanner used. SPECT study was not done as the neurologic insult had been of very long duration. Case 2 : PA, 14 years female, was first seen in June 2000 for treatment of spasticity. Details of her birth history were not available; however, reduced movement of left limbs was noted quite early (less than one year age). Her milestones were delayed and dragging of left leg was noted. She started walking at around two and half years of age. She was found to be grossly mentally retarded and developed marked behavioral problems over the years. She had few seizures early in life with fever but thereafter these did not recur. Examination revealed a retarded girl with slurred speech, left hemiparesis and marked spastic dystonia of the left limbs. The left hand and foot were considerably smaller than the right. MRI of brain (Fig. 3) revealed gross hemiatrophy of the right hemisphere with considerable dilatation (compensatory) of the right lateral ventricle and widening of the overlying subarachnoid space. The right cerebral peduncle was considerably atrophied. The left cerebellar hemisphere showed considerable volume loss. Hemispheric volumetry was not possible. Discussion Both the aforementioned cases can be taken as examples of infantile hemiplegia syndrome. Case 1 had features of the hemiplegia - hemiatrophy - hemiconvulsion (HHH) syndrome but seizures had not been a major problem in case 2, who was considerably more handicapped physically. The etiology of the cerebral injury remains unclear, but the possibility of a vascular injury early in life is most likely. MRI in both revealed unilateral cerebral hemiatrophy; atrophy of the ipsilateral cerebral peduncle (suggesting degeneration of ipsilateral cortico-bulbar and cortico-spinal tracts) and volume loss in the contralateral cerebellar hemisphere. The latter finding would suggest structural cerebral affection as a result of injury to the contralateral cerebral hemisphere i.e. crossed cerebral cerebellar diaschisis (CCD). Case 2 undoubtedly had a more marked cerebral hemiatrophy and this has been reflected on more obvious atrophy of the ipsilateral cerebral peduncle and greater volume loss in the contralateral cerebellar hemisphere. This observation would be in concordance with the concept CCD. However, inspite of marked cerebellar volume loss in one hemisphere, none of the cases showed any clinical evidence of cerebellar disease. The significant motor deficit and spasticity undoubtedly masked any cerebellar component in the clinical evaluation. Hamano et al,3 studied 25 patients of CCD. Seven had cerebral palsy and the others had brain injury between 10 months and 14 years of age. CCD (hypoperfusion on SPECT) was demonstrated in 5 patients (20%), who acquired brain injury after 7 years of age. CCD was not be detected in patients with cerebral palsy. Ipsilateral cerebellar diaschisis was also demonstrable in two patients with cerebral palsy and in three with early acquired brain injury before 3 years of age. The authors suggested that diaschisis (manifested by hypoperfusion) presents itself as a different form (ipsilateral or contralateral) depending upon the age of cerebral insult. Early insults would be likely to produce ipsilateral and the later ones to produce a crossed cerebellar diaschisis. The same observation had been made by the authors later on, by SPECT studies on a larger number of children with hemiplegic syndromes.4 Sztriha et al5 also observed similar findings. CCD has been demonstrated by SPECT study in a young boy with basal ganglia germinoma which improved after therapy of the offending lesion.6 CCD has also been studied in adults with hemispheric brain injury by functional neuroimaging (SPECT) in various conditions including Alzheimer's disease,7 ischemic cerebrovascular disease,8-11 cerebral hematomas,12 brain tumors,13 head injury14 and epilepsy.15 None of the studies quoted above, have however, mentioned about morphological changes observed in the cerebellum as a result of CCD. The present report appears to be significant in this respect that in both subjects, evidence of cerebellar volume loss could be detected on MRI, contralateral to the side of cerebral lesion. Furthermore, there appears to be some correlation between the degree of morphologic damage to the cerebrum and the volume loss in the opposite cerebellum. Tien and Ashdown commented on such morphological alteration in the cerebellum on MRI and reported similar correlation.16 Both the reported cases herein, appear to had the cerebral insult quite early in life (before 1 year of age) and both showed evidence of CCD morphologically. In view of this observation, the author would argue against the opinion expressed by Hamano et al3,4 that early cerebral injury would be more likely to produce ipsilateral rather than contralateral cerebellar diaschisis. In this connection, the studies by Shamofo and Chugani17 and Niimura et al18 seem noteworthy. These workers, using PET, demonstrated increased glucose utilization and increased binding of benzodiazapine receptors in the contralateral cerebellar hemisphere when brain injury occurred early in life before one year of age but after the first 4 weeks. This had been the case with both the patients cited in this communication. It appears that the increased metabolic rate perhaps signifies nature's defence mechanism to prevent neuronal damage in the contralateral cerebellum following cerebral injury. With increasing age, this increased metabolic rate is likely to die down and morphological evidence of neuronal loss becomes evident. Imaging done later in life, therefore, showed contralateral cerebellar volume loss. It is to be noted, that this increased metabolic rate could not be demonstrated in older children and in adults on SPECT (vide supra). Naturally, there is difference in cerebellar functional reorganization pattern following contralateral cerebral injury between developing and developed brains. Recently, Gasparini19 et al described a patient with linguistic impairment (without any other cognitive dysfunction) after a right cerebellar stroke. Though SPECT study showed gross hypoperfusion in the affected cerebellum, no perfusion alteration (diaschisis) could be demonstrated in the opposite cerebral hemisphere. In contrast, Broich et al20 demonstrated SPECT evidence of contralateral cerebral hemispheric hypoperfusion following a right cerebellar infarction. Such studies are expected to throw considerable light on the non-motor functions of the human cerebellum. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02092f1.jpg] [ni02092f2.jpg] [ni02092f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}