 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 326-329 Benign Meningioma Metastasizing through CSF Pathways : A Case Report and Review of Literature T.V. Ramakrishnamurty, A.V.R. Murty, A.K. Purohit, C. Sundaram* Departments of Neurosurgery and Pathology*,
Nizam's Institute of Medical Sciences,
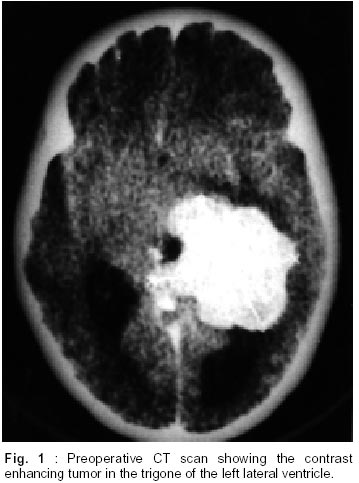
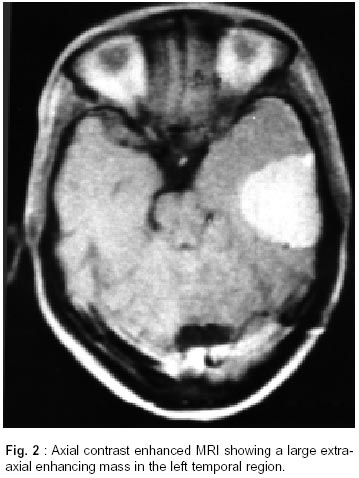
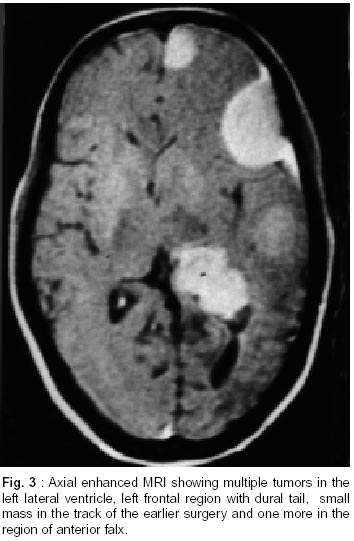
Panjagutta, Hyderabad - 500 082, India. Accepted for publication : 21st December, 2000. Code Number: ni02093 Summary Metastasis of intraventricular meningiomas through CSF pathways is a rarity and only 4 cases have been reported in world literature describing meningiomas which were intraventricular and malignant. Here we report a case of benign intraventricular meningioma which had spread through CSF pathways, the recurrences as well as the primary tumor being benign in nature. Key words : Intraventricular, Meningioma, Metastasis, Cerebrospinal fluid. Introduction Meningiomas are common tumors and constitute 14-20% of all intracranial tumors. Meningiomas which are purely intraventricular in location are rare and constitute about 0.7% of all intracranial tumors. Metastasis of meningiomas to distant extracranial sites is well known. The spread is supposed to be through blood borne route. The metastasis of meningiomas through the CSF pathways is rare, although these tumors which arise from the arachnoid cap cells, develop in close proximity to the CSF pathways.1 The metastasis of intraventricular meningiomas through CSF is still rarer and only four cases have been reported in the world literature after undergoing surgery. In all the cases, the original tumor had a malignant histology at the time they underwent surgery for the metastasis. Here we report a case of a meningioma which was intraventricular in location and was benign in nature. Four years later there were multiple recurrences which were benign at the second surgery as well. The term 'benign metastasis' coined by Som et al in 1987 is, hence, worthwhile.2 Case Report A 22 year old lady seen in November 1994 with complaints of localized headache in the left frontoparietal region. Headache was associated with vomitings. On examination, there was bilateral papilledema and no other focal deficit. CT scan of the brain revealed a large hyperdense lesion in the left trigone region of the left lateral ventricle. There was no calcification. Mild ventriculomegaly was present. The lesion was brilliantly enhancing with contrast (Fig. 1). Patient was operated in November 1994 and a large meningioma in the trigone of the left lateral ventricle was totally excised. Histopathological examination of the mass was reported as a transitional meningioma. Patient was under regular follow up. A routine CT scan of the brain done in 1997, 3 years after the surgery revealed a small recurrent tumor in the left trigone region, which was enhancing with contrast. In May 1998, she again presented with severe headache localized to the left frontoparietal region and a single episode of right focal seizure with secondary generalization and post ictal paresis for 24 hours. Examination revealed bilateral papilledema with grade IV hemiparesis on the right side. CT of brain with contrast administration revealed multiple hyperdense lesions in the left hemisphere. Two lesions were located in the left frontal region, one each on the anterior falx, in the pterional region, temporal region and the parietal region. There was a large recurrence of the intraventricular mass in the left trigone region. All the lesions were brilliantly enhancing with contrast. MRI study of the brain also confirmed the CT scan findings (Fig. 2 and 3). An extended fronto temporo parietal craniotomy was done on the left side. The brain was studded with multiple meningiomas of different sizes. All the lesions were totally excised. The gliotic plane of the earlier approach to the trigone had three small meningiomas which were also excised. The intraventricular meningioma was also totally excised. Histopathological examination revealed sheets and bundles of meningothelial cells forming whorls. Cells had acidophilic cytoplasm and an elongated vesicular nucleus. The intraventricular lesion showed frequent mitoses. No areas of necrosis or pleomorphism were seen. The tumors were, thus, of the transitional variety with no evidence of malignancy. Discussion Meningiomas constitute 14-20% of all intracranial tumors.1 Usually, most of the tumors are benign. The malignant group constitutes less than 10% of the entire group of meningiomas.3 0.7% of all tumors occur in the intraventricular compartment. Medulloblastomas, ependymomas, glioblastoma multiforme, pinealomas and malignant choroid plexus papillomas are known to spread through CSF pathways. Meningiomas arise from the arachnoid villi, tela choroidea or leptomeninges and invariably face the CSF. Seeding of meningiomas to the extraneural organs is seen, but seeding through CSF pathways is rare, inspite of the fact that they are closely situated in relation to the CSF pathways.1 The incidence of meningiomas occuring in the lateral ventricle has been variably reported between 0.7 to 2% of all intracranial meningiomas.4-6 Kepes in 19827 reviewed the literature and collected 12 cases of metastasis in cases of meningiomas which had spread through CSF pathways. Six had metastasis in the spinal region or cauda equina. Miller and Ramsden8 suggested that the dynamics of the system might prevent settlement of cells but have assumed that the existence of an antimeningioma antigen is unlikely in the cerebrospinal fluid, as it occurs in other organs. The reason of low spread through CSF is still not clearly elucidated. It has been conclusively proved that they may not metastasize unless they have formed jointed fragments.8 A review of the previously reported cases shows that two of them arose in the left lateral ventricle, one in the right lateral ventricle and the one in the third ventricle. One patient had multiple cerebral metastases,3 one had a single spinal deposit9 and one patient had multiple deposits in the medulla, cerebellum, pineal and spinal cord.10 The fourth case had a lumbar deposit and also bilateral cerebellopontine angle deposits.11 All the above mentioned cases underwent surgery after the appearance of metastases and were histologically proved as malignant meningiomas. Hence, the previously proposed theory that surgery is the cause for the dissemination was negated since the incidence is so low in the face of so many tumors being operated and also because of the fact that malignant meningiomas can spread without prior surgery. Total six cases were found on reviewing the world literature on metastasis of extraventricular meningiomas. In three cases, the primary and metastases were believed to be completely benign.12,13 In the other three cases, the primary and the metastasis were supposed to be benign but the histological confirmation was not present in these cases.2 These cases have therefore been called as 'Benign Metastasis'. The case reported here is different from the above cases in the sense that it was originally an intraventricular tumor in the trigone of the left lateral ventricle which had developed metastases through the CSF pathways. The primary as well as the metastases are entirely benign. However, the metastases might be initially benign in nature but become progressively malignant as it recurs again. Hence, radiation therapy in these patients might be justified, inspite of total excision of all the metastatic tumors. In the present case, the location of the tumors also confirms that surgery might have been the cause for the spread of the metastasis since small meningiomas were found in the gliotic plane of cleavage in the path which was taken for the first surgery. All the tumors were located on the side of the surgery without any distant foci of metastasis. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02093f2.jpg] [ni02093f3.jpg] [ni02093t1.jpg] [ni02093f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}