 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 334-336 Case Report Adult Atretic Parietal Cephalocele S. Abubacker, B. Lakhkar, D. Shetty, G. Krishna Department of Radiodiagnosis and Imaging,
Kasturba Medical College
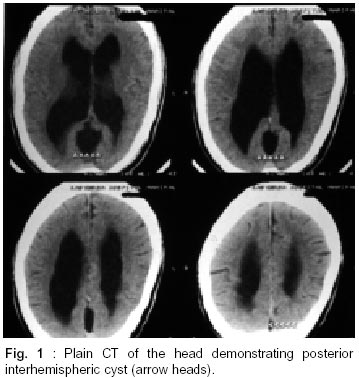
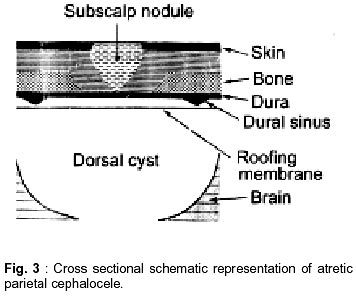
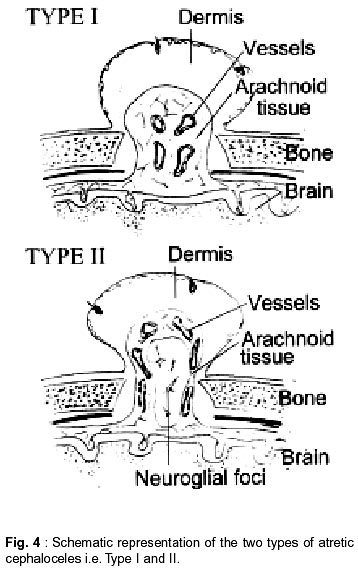
Manipal - 576 110, Karnataka, India. Accepted for publication : 30th January, 2001 Code Number: ni02095 Summary Atretic parietal cephalocele is a congenital anomaly of childhood with poor prognostic value. The authors report an adult with associated brain malformations (interhemispheric cyst, partial corpus callosum agenesis) - but, interestingly, without any clinical symptoms related to the entity. Key words : Cephalocele, Parietal, Atretic. Indroduction Atretic parietal cephalocele is an abortive form of meningomyelocele. It refers to a skin - covered subscalp lesion that consists of meninges and rests of glial and/or CNS tissues.1 It is a childhood anomaly with poor prognosis.2 The children are either retarded or die at an early age. Review of literature revealed only one such case in an adult, who had no associated malformations.3 We report a case of atretic parietal cephalocele in an adult, with associated malformations, who had 'normal mental development'. CT and MRI morphologies of this entity are described. Case Report A 63 year old man with history of mitral stenosis presented with acute onset abnormal behaviour. He was referred from the psychiatry department for a CT scan of the head to rule out a vascular event due to embolization. Plain CT scan of the head revealed a subscalp nodule arising in the parietal area posteriorly and in the midline with an underlying bone defect. CT also revealed an inter-hemispheric cyst situated in the mid-line posteriorly (Fig. 1). Post-contrast CT showed enhancement of the nodule. MRI showed the sub-scalp nodule with an underlying bony defect. The margins of the defect were seen to narrow from inside outwards. Associated abnormalities noted on MRI were a posterior inter-hemispheric cyst and partial agenesis of the corpus callosum (Fig. 2). Clubbing all the imaging features and the skin changes over scalp i.e. an alopecic area, well marginated and covered with atrophic skin, a final diagnosis of 'atretic parietal cephalocele' with underlying malformations was made. Discussion Cephaloceles are congenital herniations of intracranial structures through a skull defect.4 Parietal cephaloceles are uncommon, comprising approximately 10% of cephaloceles.5 James and Lassman6 introduced the concept of an abortive form of meningomyelocele in 1972 and termed it 'meningocele manqué', meaning spontaneous arrest in the development of the malformation. Other expressions for this entity are 'abortive' and 'atretic' cephalocele referring to a skin covered subscalp lesion that consists of meninges and rests of glial and/or CNS tissues. It is interesting to note that a high percentage of parietal cephaloceles fall into this atretic category.2 Atretic parietal cephaloceles present clinically as a hairless well marginated round scalp lesion covered with atrophic skin. Initially after birth they are cystic but within several days they are transformed into a flat alopecic lesion.1 They are usually associated with a hole in the underlying skull and the lesion is separated by the dura from the underlying brain, where a dorsal cyst abuts in a majority of cases (Fig. 3). In our patient there was an alopecic area in the posterior parietal midline, well marginated and covered by a parchment - like membrane. The underlying defect could be felt on palpation. Based on pathological features atretic cephaloceles are classified into two categories.1 in Type I cephalocele the lesion consists mainly of arachnoid tissue found at the lesion stalk and is accompanied by a cluster of anomalous blood vessels. The dome consists of dermal tissue with normal hair follicles (Fig. 4). In Type II cephaloceles (Fig. 4), the blood vessels extend towards the lesion dome and in this variety ectopic foci of neural/glial elements are also seen. The blood vessels, account for the enhancement patterns seen in both, Type I and II. Atretic parietal cephaloceles have a very high incidence of associated midline anomalies, including porencephalies, interhemispheric cysts and callosal agenesis.5 It is because of these associations that the atretic parietal cephalocele has a very poor prognosis - most of the children dying retarded.2 In our case it is interesting to note that inspite of being associated with these malformations the patient had a normal mental development during his childhood and the findings were totally incidental, being discovered at 63 years of age. Plain skull radiographs1 demonstrate an underlying bone defect in the area of the cephalocele with welldefined margins measuring 0.5 - 1.5 cm in diameter. The margins are occasionally sclerosed and the defect is oval or elongated in shape. In our case a plain skull radiograph was not taken. CT images revealed a subscalp nodule with a density close to CSF or slightly hyperdense to brain parenchyma.1 Postcontrast images revealed enhancement of the nodule attributed to the anomalous vessels present within. The underlying bone defect can be seen with margins tapering from inside outwards which is important to differentiate it from an overlying dermoid cyst in which case the bony margins taper from outside inwards. Associated malformations like underlying inter-hemispheric and porencephalic cysts can be picked up by CT. MRI, especially in the sagittal plane, demonstrates the subscalp nodule, underlying calvarial defect with characteristic margins and associated malformations especially corpus callosum agenesis which is easier to pick up on MR as compared to CT.1 Our case showed all the above CT and MRI features. The differential diagnosis include dermoid cyst and sinus pericranii. Dermoid cysts on a plain skull radiograph7 shows a rounded defect with partially sclerosed margins as opposed to atretic cephalocele where the defect is oval or elongated. The edges of the dermoid cyst on CT narrow from outside inwards, the opposite being seen in atretic cephalocele, in which case the margins narrow from inside outwards. Dermoid cysts do not enhance with contrast where as atretic cephaloceles enhance vividly.1 Sinus pericranii are soft bulging masses in the scalp situated close to the midline which can be seen in the parietal area.8 They represent dilated veins that communicate with the dural sinuses by way of an emissary vein. Clinical findings include a subscalp soft tissue tumor that empties when the patient is standing and refills when the patient is lying down. Imaging studies9 will show a soft tissue mass that enhances after contrast infusion and is accompanied by scalloping of the outer table of the skull. Sagittal MRI shows its relationship to the underlying dural venous sinus. To conclude, atretic parietal cephaloceles, though believed to be an abortive form of meningomyelocele, represents only the 'tip of the iceberg'. CT and MR image morphology is required to make a diagnosis of the underlying malformations. The presence of these malformations do not necessarily add to the bad prognostic value as seen in our case. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02095f3.jpg] [ni02095f2.jpg] [ni02095f4.jpg] [ni02095f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}