 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 50, No. 3, Sept, 2002, pp. 352-358 Case Report Choroid Plexus Papillomas of the Cerebellopontine Angle Raj Kumar, G. Achari, D. Banerji, V.K. Jain, D.K. Chhabra Department of Neurosurgery,
Sanjay Gandhi Postgraduate Institute of Medical Sciences,
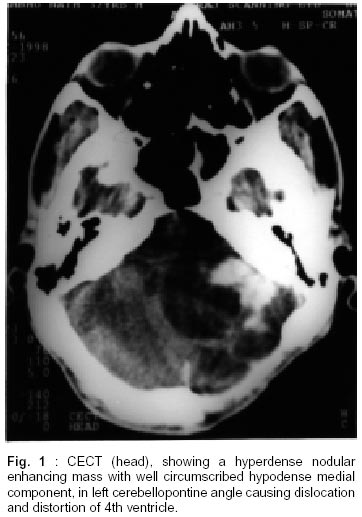
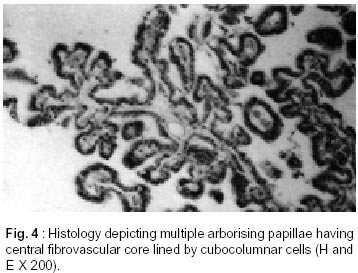
Lucknow - 226 014, India. Accepted for publication : 20th July, 2000. Code Number: ni02099 Summary The cerebellopontine angle (CPA) is a rare site for the growth of choroid plexus papilloma (CPP). The clinicoradiological diagnosis of this tumor in the CPA is difficult because of the nonspecific clinical presentation and radiological features. Five cases of choriod plexus papilloma (3 males, 2 females) operated upon at this center are reviewed. All the cases were operated upon by retromastoid suboccipital craniectomy. As they all presented with a typical CPA syndrome without any distinctive radiological feature, a clinicoradiological diagnosis of CPP could not be reached in any of these. The diagnosis of CPP could only be suspected at the operation table and established on histopathological examination. Two patients developed recurrences at the primary site following surgery. One patient developed recurrence twice despite gross total excision of tumor in each sitting. Subsequently, this patient remained symptom free for a follow-up period of 1 year. Another patient developed recurrence 2 years following surgery, but he died due to septicemia and aspiration pneumonitis. Therefore definitive surgery could not be performed. Radiotherapy was offered to one of the patients having residual mass post operatively, to render her symptom free for a 4 year follow-up. The remaining two patients have also showed progressive improvement in their symptoms following surgery for 4 years on follow-up. Hydrocephalus was a common feature in all the cases preoperatively, but only one required shunt CSF diversion, because of rapid deterioration in visual equity. In all other cases, hydrocephalus was managed conservatively. Surgery remains the main modality of treatment for CPP, both for primary and recurrent tumors, but radiotherapy may have a role in cases of recurrence, which are quite frequent. Key words : Cerebellopontine angle, Choroid plexus papilloma, Radiotherapy. Introduction Choroid plexus papillomas (CPP) are benign slow growing tumors of neuroectodermal origin. Their incidence among all intracranial neoplasm, at all ages, varies between 0.4% to 1%.1,2 Incidence amongst children is greater (1.5% to 4%), with a peak in first two years of life.2,3 They are less frequent in adults, comprising 0.3% to 0.89% of intracranial tumors.3 Common sites of these tumors are lateral ventricles in children and fourth ventricle in adults.2,4,5 The tumor arises exclusively within the ventricle (92%) in children.6 The cerebellopontine angle and the third ventricle are extremely rare sites for primary choroid papillomas.7-9 Total microsurgical resection of this tumor is mandatory to reduce the incidence of recurrence. Although these tumors are benign, yet they have a tendency to metastasize,7,10,11 and undergo malignant transformation. We report a series of five cases of primary cerebellopontine angle choroid plexus papillomas operated from 1991 to 1999. Material and Methods Five cases of primary choroid plexus papilloma of the cerebellopontine angle, operated between 1991 and 1999, in the department of neurosurgery, were reviewed. The initial clinicoradiological details of these cases were recorded from their case sheets. The radiological data was re-evaluated and follow up was ensured once the diagnosis of choroid plexus papillomas was established on the operation table and by histopathological examination. Preoperative plain and contrast CT scan was available in all the cases. Postoperative CT studies were used to document the totality of excision in 4 cases. Hydrocephalus was present in these patients, but only one patient required ventriculoperitoneal shunt. The histopathology of all five cases was classical of benign CPP, including the specimens examined following reoperation for recurrences. All the tumors were approached by retromastoid suboccipital route. Case Report Case 1 : A 31 year old male was admitted in neurosurgery department in August 1996, with four months history of swaying to the left and loss of taste sensations on left half of tongue. Headache and vomiting were present for the last one month. Neurological examination revealed bilateral secondary optic atrophy, perception of light in both eyes, bilateral 6th nerve paresis, left 7th nerve paresis of LMN type, gross sensorineural deafness in left ear and pronounced left sided cerebellar signs. Pure tone audiometry showed 45 db hearing loss in left ear, while BERA revealed the delayed latencies of waves I to III and I to V. Plain and contrast CT scan showed a hypo to hyperdense irregular, large, heterogeneous CP angle (left) mass with nonhomogeneous enhancement on contrast, compressing the brain stem, shifting the 4th ventricle to contralatral side and extending to foramen of magnum (Fig. 1). During surgery, the tumor had a large cyst containing xanthochromic fluid in the region of the foramen of Luschka and brainstem with a solid component projecting laterally, away from brainstem. The cyst was decompressed and solid part was completely excised. Seventh nerve and the ower cranial nerves were seen on anterior aspect of mass and preserved. On histopathological examination, multiple delicate papillary structures displaying attenuated cell lining at most places, with flattened to cuboidal cells at other places, were seen. Numerous variable size vessels and dense fibro collagenous tissue were documented. Surrounding brain parenchyma displayed gliotic changes. In the immediate post operative period, the patient developed meningitis which was successfully treated. A bulge developed at the operative site which responded to repeated lumbar CSF drainage and acetazolamide therapy. At discharge he had left-sided cerebellar signs along with left 6th nerve paresis, left 7th nerve palsy, complete left sided sensorineural deafness and blindness due to secondary optic atrophy. The patient showed progressive improvement in cerebellar signs during follow-up. Two years later, in December 1998, he developed persistent headache and recurrence of left sided cerebellar signs. Hoarseness of voice and difficulty in swallowing due to lower cranial nerve involvement became evident. He also had the pre-existing bilateral secondary optic atrophy, left seventh nerve palsy, left lower cranial nerve paresis with gross left sided cerebellar signs. A repeat CT scan showed a large cystic recurrence in the left cerebellopontine angle (Fig. 2). He was advised surgery, but developed aspiration pneumonitis and septicemia and succumbed before any operative intervention. Case 2 : A 32 year old female was admitted in December 1995 with history of progressive hearing loss in the right ear for 7 months. History of severe episodic headache, diplopia and progressive diminution of vision for one and a half months was also reported. Her examination revealed bilateral papilloedema, 20% hypoesthesia in right V1 and V2 distribution of 5th nerve, right sided 6th and 7th nerve paresis, right sided sensorineural deafness and gross right cerebellar signs. Pure tone audiometry showed hearing loss of 60 db in right ear with absent BERA on right side. The CT scan showed an isodense mass with heterogeneous contrast enhancement in right cerebellopontine angle. It was a large, 4x5 cm mass without an extension into the internal auditory meatus. Fourth ventricle was dislocated to the contralateral side causing obstructive hydrocephalus. On exploration, the tumor had a large cystic component present posteriorly and a solid component with a poorly defined plane of cleavage; it was a soft vascular and suckable mass attached to the brain stem in the vicinity of foramen of Lushka. It was also extending out through the jugular foramen. Fifth, sixth and lower cranial nerves were recognized and preserved, though these were found to be stretched by the tumor. The seventh nerve was enmeshed within the tumor and hence, could not be saved. Histopathology showed papillary structures with delicate fibrovascular core lined by columnar cells with vesicular nuclei, which is typical of choroid plexus papilloma. Following surgery, headache became less intense and less frequent, cerebellar signs also improved. At three months' follow-up, she had complete recovery of headache, right cerebellar signs and 6th nerve paresis. She had only 5-10% hypoesthesia in V1,V2 distribution of 5th nerve. However there was no improvement in her hearing and 7th nerve functions. Three years later, her right cerebellar signs reappeared and facial numbness intensified, headache and difficulty in swallowing also became worse. Neurological examination revealed 75% hypoesthesia in V1 and V2 distribution of right 5th nerve, right 7th nerve palsy, right sided gross sensorineural deafness, paresis of 9th, 10th and 11th nerve, with gross cerebellar signs on the right side. A repeat CECT head showed a large hypodense homogeneously enhancing mass in right CPA (Fig. 3). On re-exploration of retromastoid craniectomy, a soft to cystic vascular mass with a poorly defined plane of cleavage from the brain stem was encountered. Neartotal microsurgical excision of the mass could be done without further compromise of cranial nerves/brain stem. Following surgery, despite initial improvement in headache, her residual symptoms remained persistent. A repeat CT scan, 4 months later, showed a large recurrence at the same site. Surgical excision of a vascular mass with simultaneous fulguration of the choroid plexus in the region of foramen of Luschka could be achieved. There was improvement in facial hypoesthesia and cerebellar signs in post operative period. She developed a bulge at the operative site due to CSF collection which could be managed with repeated lumbar CSF drainage and acetazolamide therapy during hospital stay. Three months later, on follow up, she showed further improvement in gait and had only 5 to 10% hypoesthesia in V2 and V3 distribution. She was symptom free at one year follow-up. Case 3 : A 40 year old male presented with a one year history of mild to moderate holocranial headache, which had increased in frequency and intensity for the last 4 months and was associated with vomiting. He also developed unsteady gait and swaying towards the right side. Occasional diplopia on left lateral gaze and heaviness of voice was also noticed. On examination, he showed bilateral papilledema, bilateral 6th nerve paresis, horizontal gaze evoked nystagmus and right sided cerebellar signs. Laryngitis and incidental vocal cord nodule were found on throat examination. CT scan showed hyperdense enhancing lesion of 3 cm x 4 cm at right cerebellopontine angle with an arachnoid cyst and a broad based dural attachment to the petrous. Fourth ventricle was shifted to left causing a mild obstructive hydrocephalus. On MRI the mass was extending into the foramen of magnum. It was hypointense on T1 and hyperintense on T2 with a cystic component encircling the tumor inferiorly. The right CPA cistern was dilated, brain stem was compressed and shifted towards opposite side by the tumor. Right 7th and 8th nerve complex was separate from the mass. Pure tone audiometry demonstrated mild bilateral sensorineural deafness with brain stem evoked responses of prolonged inter peak latencies between wave I to III and III to V. A clinical diagnosis of right CPA meningioma was considered on initial work up and the tumor was approached by right retromastoid suboccipital craniectomy. On exploration of the CPA, the mass was soft to firm, partly suckable, vascular with a well-defined capsule, good arachnoid plane and had an arachnoid cap. It was adherent to rootlets of lower cranial nerves and partly to 7th and 8th nerve complex. Complete microsurgical excision, while preserving 7th, 8th and lower cranial nerves, was achieved. A histological diagnosis of choroid plexus papilloma was made (Fig. 4). Hoarseness increased in post operative period, which on conservative management improved gradually. He developed meningitis 3 weeks after surgery, which was managed by oral antibiotics. On discharge, there was improvement in gait, diplopia and nystagmus. He had mild residual cerebellar signs particularly gait ataxia at six months follow up. He was symptom free at 4 years follow-up. Case 4 : A 32 year old male patient presented with 8 months history of progressively increasing holocranial headache and 6 months history of bilateral visual deterioration. He had an unsteady gait with a tendency to sway towards left and diminution of hearing from left ear for 2 months. Visual acuity was 6/60 in both eyes with bilateral gross papilledema. An absent corneal reflex and mild cerebellar signs were demonstrated on left side. Pure tone audiometry showed mild left sided sensorineural deafness having 35 db loss and no wave form on BERA of ipsilateral side. CT scan showed a large hyperdense mass, with areas of calcification, enhancing on contrast, occupying the whole of left CPA cistern and partly extending into the fourth ventricle through a probably dilated foramen of Lushka. A clinicoradiological possibility of an ependymoma was kept, a right ventriculoperitoneal shunt was done because of the visual threat to the patient. Left retromastoid suboccipital craniectomy, revealed a grayish, pink soft vascular mass in left CPA extending through the foramen of Lushka into the fourth ventricle (with only a small intraventricular component). Lower cranial nerves were enmeshed in the tumor, but they could be separated and preserved along with the 6th, 7th and 8th nerves, which were also stretched by the mass. Histopathology of specimen revealed the diagnosis of choroid plexus papilloma. Post operatively, the patient showed improvement in headache and cerebellar signs but vision did not improve because of setting in of secondary optic atrophy. Case 5 : A 32 year old female was admitted with complaints of gradually progressive diminution of hearing and occasional tinnitus of four years duration. She was also bothered by increasing frequency and severity of left hemifacial spasm during the last 6 months. Her examination revealed left seventh nerve : lower motor neuron paresis and left sided sensory motor deafness. There was no evidence of increased intracranial tension. CT scan revealed a low attenuating lesion in left cerebellopontine angle with destruction of petrous bone and widening of left internal acoustic meatus. MRI was done to confirm the CT findings. In addition, it showed the extension of the lesion upto jugular foramen inferiorly and tentorium superiorly. Four vessel digital subtraction angiography was considered to rule out vascular lesion, which suggested a left CPA lesion without vascularization of lateral/transverse sinus. She underwent elective left retromastoid suboccipital craniectomy. A well demarcated vascular lesion extending from foramen magnum and jugular foramen was seen in left CPA. The tumor contained brownish fluid and soft tissue, petrous bone was destroyed. Partial microsurgical decompression was achieved and tarsorrhaphy was done on left eye. She was discharged on 4th postoperative day. Frequency of left hemifacial spasm reduced. The specimen on histopathological examination established the diagnosis of choroid plexus papilloma. The immunological staining for glial fibrillary acidic protein was negative, excluding the possibility of a papillary ependymoma. She was subjected to radiation therapy for residual tumor mass. Craniospinal irradiation was planned and a dose of 54 Gy in 30 fractions to the whole brain and 30 Gy in 18 fractions to spinal cord were given. The whole treatment lasted 10 weeks. She tolerated the therapy well and remained disease free for 4 years. Discussion Choroid plexus papillomas are rare intracranial tumors of neuroepithelial origin, accounting for 0.4% - 1.1 % of all intracranical tumors.1,2 They usually occur in the first and second decades of life but have been reported in other age groups as well.26 Choroid plexus tumors commonly occur in the lateral ventricles in children1,2 and in the fourth ventricle in adults.4 The cerebellopontine angle is rarely affected. In a series of 245 patients of choroid plexus papillomas, only 17 were located in the cerebellopontine angle.6,9 There are 6 other cases of histologically proven choroid plexus papillomas in the CPA.10 Origin of CPA choroid plexus papilloma remains a point of speculation. The choroid plexus of fourth ventricle extends through the foramen of Lushka into the CPA and is known as the Bochdalek's basket. This is implicated as the site of origin of choroid plexus papilloma.12,13 Dysfunction of hearing, facial movements and sensation, cerebellar signs, gait ataxia, dysarthria, papilledema and blindness are common presentations of CPP in CPA.12 A rare case of choroid plexus papilloma presenting as a subarachnoid hemorrhage with intraventricular bleed has also been reported in literature.14 The clinical syndrome of CPA dysfunction occurs in a number of other common tumors in this location. Thus it is difficult to arrive at a clinical diagnosis of choroid plexus papilloma occupying CPA at many occasions, even after MRI study. None of the patients from the current discussion was clinically diagnosed as a case of CPP. The differential diagnosis remained acoustic schwannoma for case 1 and case 2, meningioma in case 3 and ependymoma for case 4. Predominant involvement of 8th and 7th nerve in case 1,2, and 5 favoured a diagnosis of acoustic schwannoma, while homogeneous enhancement on contrast in case 3 favoured a diagnosis of meningoma. An enlarged foramen of Lushka and extension of tumor into the fourth ventricle favoured a diagnosis of ependymoma in the fourth case. The typical CT picture of choroid plexus papilloma has been described as a well defined homogeneously enhancing mass with lobulations and frond like irregular pattern resulting in a cauliflower like appearance.15 It is typically seen in cases of intraventricular sites of this tumor. In the five cases reported here, the tumor mass was hyperdense, enhancing on contrast but without frond like pattern, described for intraventicular locations of choroid plexus papilloma. Calcifications were seen in only one case and no evidence of extension into internal auditory meatus was seen. Extension into the jugular foramen was seen in only one patient and to the foramen magnum in two patients. However, Mc Girr16 reported 20% calcification and Rovit et al9 reported 4.1% incidence of calcification in their series. With absence of frond like pattern, calcifications and enlargement of foramen of Luschka, a radiological diagnosis of choroid plexus papilloma in the CPA is difficult. MRI may reveal isointense lesion on T1WI and iso to hypointense lesion on T2WI with marked enhancement on contrast study.15 MRI can give a better anatomic delineation and may rule out other tumours like acoustic schwannoma. Absence of an intra canalicular extension into the internal acoustic meatus, may help in ruling out an acoustic schwannoma, even though the destruction of petrous and erosion of IAM have been reported in cases of CPA choroid plexus papilloma.8 Epidermoid in CPA can also be ruled out by using T2WI and PD sequences on MRI, by the interdigitating conformity to the local space in the basal cisterns.17 A coronal section of MRI through the foramen of Luschka is recommended to diagnose a case of choroid plexus papillomas of the CPA.18,19 Blood supply of a CPA choroid plexus papilloma is virtually from the AICA and an enlarged AICA on vertebral angiography helps in diagnosis.20,21 Calcifications, broad based dural attachment and increased vascularity may mimic a meningioma.13 The tumors though benign, may be adherent to the brainstem, making total removal very difficult.8 Local invasive character of the tumor and propensity for dissemination through CSF, may lead to intracranial metastases.19 Repeated recurrences may indicate malignant transformation,22 While a case in the present series developed recurrence twice within a short span of three months, the biopsy remained benign in nature. Most patients with choroid plexus papilloma develop hydrocephalus because of either over production of CSF by the tumor or by obstruction of CSF pathway by compression on 4th ventricle.1,2,4 Spontaneous micro hemorrhages with secondary thickening of basal arachnoid and ependymitis are other accepted mechanisms to cause bilateral ventricular dilatation, despite a unilateral lesion. The persistence of hydrocephalus even after complete tumor removal is reported.1 Whether the microhemorrhages, responsible for hydrocephalus in intraventricular lesions, have similar contribution in the CPA is not well understood. It seems that hydrocephalus resolves after complete excision of the tumor in the CPA with opening of the cerebrospinal fluid pathway, unlike the persistent hydrocephalus seen even after surgery in case of intraventricular CPP. Only one patient in the present series required a shunt, that too because of visual threat, although other 3 patients with persistence of hydrocephalus developing repeated bulge at wound site, could be managed conservatively. The treatment used was repeated lumbar CSF drainage and cerebral dehydrants. Complete microsurgical excision of tumor is the optimum recommended therapy.6,10 Recurrence of these tumors can be a vexing problem. Anecdotal reports of CPA choroid plexus papilloma involving the petrous bone and responding to radiotherapy23 led to the consensus that radiation therapy may be useful for recurrent diseases.16 Case 5 of present series showed improvement following cranial irradiation, but the role of radiotherapy is yet to be established in these cases. Maria et al22 suggested the use of a combination chemotherapy for recurrent choroid plexus papilloma. Furuya et al10 championed the extended lateral suboccipital approach described by Heros as ideal for CPA choroid plexus papilloma but we used the retromastoid suboccipital approach to make an adequate surgical corridor for complete excision of these tumors. The approach was more familiar to the operating surgeon, since it is routinely used for surgery of vestibular schwannomas. Preoperative diagnosis of choroid plexus papilloma was not made in our cases. The diagnosis of choroid plexus papilloma was confirmed histopathologically in all the five cases. From the histological point of view, these tumors resemble normal choroid plexus consisting of fibrovascular stroma covered by unique layer of well differentiated cuboidal cells with round or basal nucleus.24 Microvilli, but not cilia, are typically present on the columnar cells and junctional complexes. The lesion may be difficult to distinguish from papillomatous ependymoma12,13 and a choroidal cyst at times.25 Improvement in microsurgical techniques have witnessed considerable reduction in mortality, morbidity and recurrence rates of choroid plexus papilloma, making its prognosis very good. Three of our cases of the present series are doing well following surgical excision and one patient developed recurrence twice within a short span of three months requiring re-exploration. One of our patient died of a treatable complication unrelated with the disease itself. Hence, it seems that clinicoradiological diagnosis of CPA - CPP is very difficult as the radiological pattern described for intraventricular locations of these tumors is not consistent with that seen in the tumor in CPA. Hydrocephalus did not warrant a CSF diversion in any of the cases in the present series and could be managed successfully on conservative lines. References
Copyright 2002 - Neurology India. Also available online at http://www.neurologyindia.com The following images related to this document are available:Photo images[ni02099f3.jpg] [ni02099f4.jpg] [ni02099f1.jpg] [ni02099f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}